
More Information
Submitted: June 02, 2022 | Approved: June 30, 2022 | Published: July 01, 2022
How to cite this article: Suzuki T, Fukumoto Y, Todo M, Tani M. A case of hemiplegia with a cerebrovascular accident in which motor imagery of finger extension on the affected side with finger extension on the unaffected side was effective - A study using F-waves. J Neurosci Neurol Disord. 2022; 6: 020-023.
DOI: 10.29328/journal.jnnd.1001063
Copyright License: © 2022 Suzuki T, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Motor imagery; Motor exercise; F-wave; Hemiplegic patient

A case of hemiplegia with a cerebrovascular accident in which motor imagery of finger extension on the affected side with finger extension on the unaffected side was effective - A study using F-waves
Toshiaki Suzuki1,2*, Yuki Fukumoto1,2, Marina Todo1,2 and Makiko Tani1
1Graduate School of Kansai University of Health Sciences, Japan
2Department of Clinical Physical Therapy, Kansai University of Health Sciences, Japan
*Address for Correspondence: Toshiaki Suzuki, Graduate School of Kansai University of Health Sciences, 2-11-1 Wakaba, Kumatori, Sennan. Osaka, 590-0482, Japan. Email: [email protected]
We investigated the effect of exercise therapy by simultaneously using motor imagery of thumb or all finger extension on the affected side and thumb or all finger extension exercise on the unaffected side by using the F-wave, which is used to measure the excitability of anterior horn cells to devise an appropriate exercise therapy using motor imagery for patients with increased muscle tone of the thumb muscles on the affected side.
Tasks 1, 2, 3, and 4 involved motor imagery of thumb extension on the affected side, motor imagery of finger extension on the affected side, motor imagery of thumb extension on the affected side based on thumb extension on the unaffected side, and finger extension on the affected side based on finger extension on the unaffected side, respectively; conducted in three trials, with one week or more between each trial. Each task was performed for one minute, with a five-minute interval between tasks. The F-waves from the thenar muscles were recorded with median nerve stimulation on the affected side before and during the tasks. The relative values of the F-wave data of the task and the F-wave data before (resting state) and during the tasks were calculated. In results, the relative data of the F/M amplitude ratio in task 4 was lower than that in the other tasks in three trials. In conclusion, motor imagery of finger extension on the affected side with finger extension movement on the unaffected side was effective for improving the muscle tone of the thenar muscles on the affected side.
Hemiplegia is observed in stroke patients. Hemiplegia treatment options include rehabilitation. Exercise therapy is one of the most commonly used rehabilitation treatments. In general, it is difficult to improve the function of the affected side of the upper limb of hemiplegic patients through exercise therapy; although there are various methods, they have not yet been established. A hemiplegic patient with a cerebrovascular accident and difficulty in voluntary movement due to severe muscle tonus in the flexor digitorum muscles on the affected side was subjected to various exercise therapies to improve voluntary movement of the affected side.
We performed imagery training to relax the flexor muscles of the thumb by using the relaxation imagery method in our previous reports [1,2]. However, no effect was observed. Moreover, we performed extension exercises on the affected side of the thumb while imagining thumb extension movement on the affected side. This exercise therapy was also ineffective. Thus, as a new trial, we performed motor imagery of thumb extension on the affected side with thumb extension on the unaffected side and found a tendency toward improvement.
To devise an appropriate exercise therapy using motor imagery for patients with increased muscle tone of the thumb muscles on the affected side, we investigated the effect of exercise therapy by simultaneously using motor imagery of thumb extension on the affected side and thumb extension exercise on the unaffected side by using the F-wave, which is used to measure the excitability of anterior horn cells.
The F-waves result from the backfiring of the α-motoneurons after the antidromic invasion of the propagated impulse across the axon hillock [3]. Its occurrence reflects excitability changes in spinal motor neurons, as reported in patients with spasticity. Analysis of F wave for excitability of spinal neural function was F/M amplitude ratio. The F/M amplitude ratio was defined as the mean amplitude of all responses divided by the amplitude of the M-wave. This is the excitability of spinal neural function compared with the excitability of muscle function.
In our previous study that investigated the nervous system of hemiplegic patients, spinal neural function excitability was evaluated using F-wave data in patients with cerebrovascular disease (CVD) [4].
In this study, we investigated whether exercise therapy with motor imagery on the affected side and voluntary movements on the unaffected side would be effective for hemiplegic patients with CVD and difficulties in voluntary movement due to severe tonus in the flexor digitorum muscles on the affected side.
The patient (60 years old, male) presented with right hemiplegia due to left cerebral hemorrhage (putamen), had increased muscle tone of the flexor digitorum muscles of the thumb (Modified Ashworth Scale 3), and had no voluntary movements of the thumb. Sensory function of affected arm was almost normal. The time post-stroke was seven years. The patient is currently undergoing exercise therapy at our clinic twice a week (20 minutes per session) for right hemiplegia. He had not received any other treatment for this disease other than exercise therapy.
We investigated the effect of exercise therapy by simultaneously using motor imagery of thumb or all finger extension on the affected side and thumb or all finger extension exercises on the unaffected side using the F-wave, which is used to measure the excitability of the anterior horn cells, to devise an appropriate exercise therapy using motor imagery for patients with increased muscle tone of the thumb muscles on the affected side.
The patient underwent exercise therapy that combined voluntary movements of the upper limb on the unaffected side and motor imagery of the upper limb on the affected side: Task 1 involved motor imagery of thumb extension on the affected side. Task 2 involved motor imagery of extension of all fingers on the affected side. Task 3 involved motor imagery of thumb extension on the affected side with thumb extension movement on the unaffected side. Task 4 involved motor imagery of extension of all fingers on the affected side with extension movement of all fingers on the unaffected side. Each task was conducted for one minute, and a five-minute break was allowed between the tasks.
The task method has been described in detail. For tasks 1 and 2, the patient was asked to imagine thumb extension (Task 1) and extension of all fingers (Task 2) on the affected side for one minute. In both tasks 1 and 2, the upper limb of the unaffected side was relaxed.
In Task 3, the patient was asked to simultaneously imagine thumb extension on the affected side and perform thumb extension movement on the unaffected side. In task 4, the patient was asked to imagine all finger extension on the affected side and perform all finger extension on the unaffected side, simultaneously.
The reason for selecting these four tasks was that the patient was unable to perform extension movements of the thumb on the affected side. Hence, we hypothesized that for a patient with such severe motor impairment, rather than simply performing motor imagery with the affected upper limb, it would be better to perform voluntary movements on the unaffected side while performing motor imagery on the affected side. We chose this option based on the framed hypothesis, which may lead to motor recovery of the affected thumb. In short, we hypothesized that tasks 3 and 4 would have a greater therapeutic effect than tasks 1 and 2. Tasks 2 and 4 were also chosen to predict whether tasks that focused only on the thumb or the entire hand helped improve the motor function of the thumb on the affected side.
For the four motor imagery tasks, three trials were conducted with an interval of at least one week.
To examine the effects of motor imagery, the F-wave, which is an index of excitability of the anterior horn cell, was conducted. The F-wave test method was as follows.
The subject was maintained comfortably in a supine position with external rotation of both shoulder joints. The skin was prepared with an abrasive gel to maintain an impedance below 5 kΩ. A VIASYS Viking Quest electromyography machine (Natus Medical Inc., CA, USA) was used to record the F-waves before and during the four tasks.
By using a pair of round disks attached to the skin and placing collodion over the belly and the bone of the metacarpal–phalangeal joint of the thumb, we tested the F-wave of the affected thenar muscles after stimulating the median nerve at the wrist before and during conditions.
The stimulating electrodes comprised a cathode placed over the left median nerve 3 cm proximal to the palmar crease of the wrist joint and an anode placed 2 cm proximally. The maximal stimulus was determined by delivering 0.2 ms square-wave pulses of increasing intensity to elicit the largest compound muscle action potentials. Supramaximal shocks (adjusted up to a value of 20% higher than the maximal stimulus) were delivered at 0.5 Hz (30 times) to obtain F-waves. The bandwidth filter ranged from 2 Hz to 3 kHz.
For the recording conditions, the exploring electrode was placed over the belly of the right thenar muscles, the reference electrode was placed on the proximal phalanx of the thumb, and the ground electrode was placed on the forearm.
The peak-to-peak amplitude of the waveform of the F-wave was measured with an oscilloscope at 0.2 mV/D. Waveforms with peak-to-peak amplitudes of 30 μV or more were judged F-waves. The peak-to-peak amplitude of F-waves that were judged to not have appeared was set to 0 μV, and the average amplitude of the 30 waveforms was calculated. The F/M amplitude ratio was defined as the mean amplitude of all responses divided by the amplitude of the M-wave.
The relative values of F-wave data were obtained during the task with respect to the before the task (resting state).
A statistical study was conducted on the relative data of the F/M amplitude ratio in tasks 1 and 3 and tasks 2 and 4 to examine the effect of voluntary movements of the unaffected upper limb on the affected thumb with paired t-test and effect size using Statistical Package for the Social Sciences (SPSS) Statistics version 26.0 (IBM, Inc., Chicago, IL, USA).
This study was conducted under the approval of the Research Ethics Review Committee of Kansai University of Health Sciences (Approval No. 19-27).
Table 1 shows the relative data of the F/M amplitude ratio in tasks 1–4. The average relative data of F/M amplitude ratio in the three trials were 0.71, 0.62, 0.69, and 0.50 in tasks 1, 2, 3, 4, respectively.
| Table 1: Relative data of F/M amplitude ratio in tasks 1-4. | ||||
| Task 1 | Task 2 | Task 3 | Task 4 | |
| Trial 1 | 0.57 | 0.25 | 0.35 | 0.26 |
| Trial 2 | 0.94 | 0.94 | 1.03 | 0.64 |
| Trial 3 | 0.62 | 0.67 | 0.68 | 0.59 |
| Average | 0.71 | 0.62 | 0.69 | 0.50 |
In the visual inspection, the relative data of the F/M amplitude ratio in task 4 tended to be lower than that in the other tasks among the three trials (Figure 1). A statistical study was conducted on the relative data of the F/M amplitude ratio in tasks 1 and 3 and tasks 2 and 4 to examine the effect of voluntary movements of the unaffected upper limb on the affected thumb. The results showed no statistically significant difference between tasks 1 and 3 and tasks 2 and 4 (paired t-test); however, the effect size was large for tasks 2 and 4 (Task 1 vs. 3: p = 0.835, r = 0.16, Task 2 vs. 4: p = 0.312, r = 0.69).
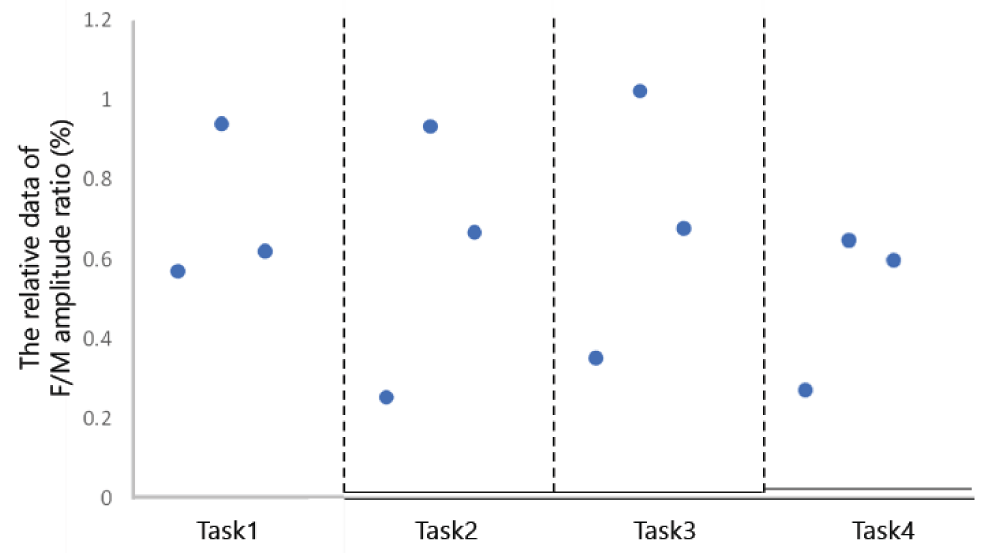
Figure 1: Relative data of F/M amplitude ratio in tasks 1-4.
Figure 2 shows a typical F-wave. Figure 2 shows the superimposed F-wave waveforms obtained for each task. The F-wave amplitude was the lowest in task 4 compared with that in the other tasks.
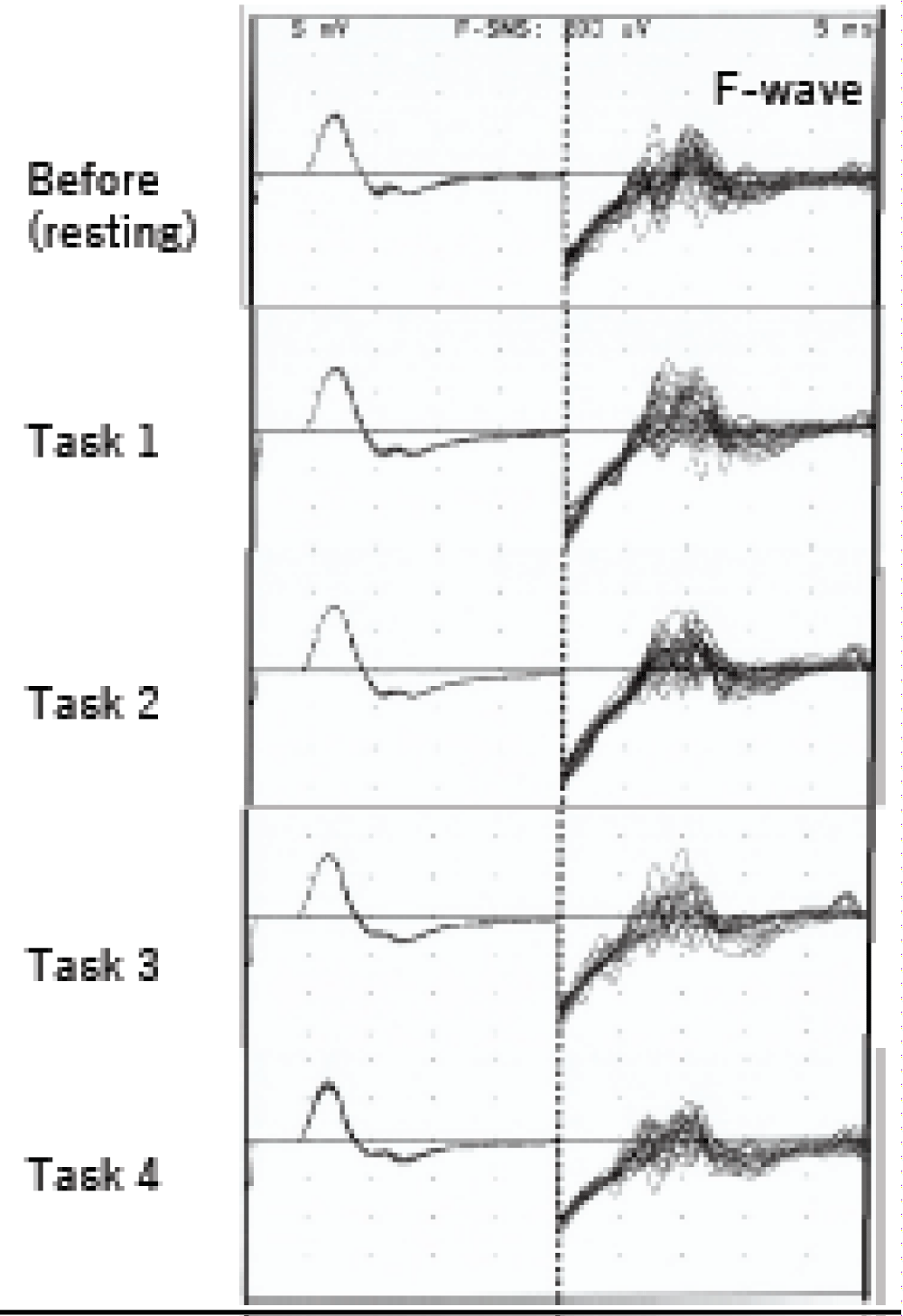
Figure 2: Typical F-wave before and during tasks 1, 2, 3, and 4.
In this case, the voluntary movement of the thumb was severely limited because of increased muscle tone of the flexor digitorum muscles of the thumb on the affected side. It was difficult to voluntarily extend the affected hand, particularly the thumb finger. Furthermore, when the patient was instructed to extend the affected side of the thumb, the affected side was characterized by increased flexion of the thumb. Therefore, we thought it would be better to perform motor imagery to extend the affected thumb than to move it spontaneously, so we performed motor imagery training on the affected side of the thumb alone. However, the effect was not obvious.
Kobayashi, et al. [5] investigated the changes in brain activity during unilateral hand movements in healthy adults by using functional magnetic resonance imaging. The results showed that blood oxygenation–dependent signals in the ipsilateral primary motor cortex and contralateral primary motor cortex increased during unilateral hand movements. Trompetto, et al. [6] measured motor evoked potentials (MEPs) in acute stroke patients by using transcranial magnetic stimulation (TMS) with cortical stimulation on the affected (contralateral), and ipsilateral sides. They reported that in patients with poor motor skills on the affected side, MEPs could not be measured contralateral and ipsilateral to the affected side.
From these two studies, it was found that bilateral brain functions are activated during voluntary movements on one side in healthy subjects, but bilateral brain functions are less activated during voluntary movements on the affected side in hemiplegic patients. Therefore, to improve the function of the upper limb on the affected side, it is important to move the upper limb on the unaffected side along with the affected side.
In the current study, the actual exercise of the unaffected upper limb and the motor imagery of the affected upper limb was performed together.
The effect of the exercise therapy was examined using the F/M amplitude ratio from the F-waves recorded from the muscle group on the affected side of the ball of the thumb by median nerve stimulation. The F/M amplitude ratio indicates the excitability of anterior horn cells (F-wave amplitude) relative to the excitability of the muscles (M-wave amplitude). The results of this study showed that the motor imagery of finger extension on the affected side with finger extension on the unaffected side decreased the excitability of anterior horn cells corresponding to the thumb muscles on the affected side. This can be explained by the fact that the motor imagery of finger extension on the affected side with finger extension on the unaffected side enabled finger extension on the affected side. This reduced the excitability of the spinal anterior horn cells corresponding to the thumb muscles on the affected side, which has a contradictory relationship.
The results of this study showed that in the F/M amplitude ratio for each task, the tendency was for motor imagery to extend all fingers on the affected side. Task 4, as well as motor imagery to extend the fingers on the unaffected side, was the most affected. Statistical examination also showed that the effect size was large when comparing the F/M amplitude ratio of tasks 2 and 4. Because the F-waves were recorded from the thumb muscle, the motor images of the extension of all fingers on the affected side, task 4, as well as the extension movements of the fingers on the unaffected side, showed a greater reduction in the anterior horn of the spinal cord corresponding to the thumb muscle on the affected side than in task 2, which simply showed the extension of the entire finger on the affected side. The number of cells corresponding to the affected thumb muscle was compared with task 2, which is simply an extension of the entire affected hand. However, the effect size of the F/M amplitude ratio of tasks 1 and 3 was small. This indicates that the effect of performing both the movement of the unaffected thumb and the extension imagery of the affected side thumb simultaneously was too small to improve voluntary movement of the affected thumb muscle.
The motor imagery of extension of all the fingers on the affected side and extension movement of all the fingers on the unaffected side may change the spinal motor neuron function in hemiplegic patients with markedly increased tone of the affected thumb flexor muscle.
In the case of no voluntary movement of the affected thumb due to hypertonia, it is useful to accompany the patient with imagery of the affected side as well as voluntary movement of the unaffected side.
Motor imagery of extension of all the fingers on the affected side and extension movement of all the fingers on the unaffected side may change the spinal motor neuron function in hemiplegic patients with markedly increased tone of the affected thumb flexor muscle.
- Suzuki T, Bunnno Y, Onigata C, Tani M, Uragami S. Excitability of spinal neurons during a short period of relaxation imagery. Open Gen Intern Med J 2014; 6: 1–5.
- Suzuki T, Bunnno Y, Onigata C, Tani M, Yoneda H, Yoshida T, et al. Excitability of spinal neurons during relaxation imagery for 2 minutes. Int J Neurorehabilitation Eng 2014; 1: 105.
- Kimura J. F-wave velocity in the central segment of the median and ulnar nerves. A study in normal subjects and in patients with Charcot-Marie-Tooth disease. Neurology. 1974 Jun;24(6):539-46. doi: 10.1212/wnl.24.6.539. PMID: 4857549.
- Eisen A, Odusote K. Amplitude of the F wave: a potential means of documenting spasticity. Neurology. 1979 Sep;29(9 Pt 1):1306-9. doi: 10.1212/wnl.29.9_part_1.1306. PMID: 573413.
- Kobayashi M, Hutchinson S, Schlaug G, Pascual-Leone A. Ipsilateral motor cortex activation on functional magnetic resonance imaging during unilateral hand movements is related to interhemispheric interactions. Neuroimage. 2003 Dec;20(4):2259-70. doi: 10.1016/s1053-8119(03)00220-9. PMID: 14683727.
- Trompetto C, Assini A, Buccolieri A, Marchese R, Abbruzzese G. Motor recovery following stroke: a transcranial magnetic stimulation study. Clin Neurophysiol. 2000 Oct;111(10):1860-7. doi: 10.1016/s1388-2457(00)00419-3. PMID: 11018503.