
More Information
Submitted: May 16, 2023 | Approved: June 20, 2023 | Published: June 21, 2023
How to cite this article: Shamsher Singh M, Gupta GD, Aran KR. Cost Variation Analysis of Various Brands of Anti-Depressants Agents Currently Available in Indian Markets. J Neurosci Neurol Disord. 2023; 7: 017-021.
DOI: 10.29328/journal.jnnd.1001076
Copyright License: © 2023 Shamsher Singh M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Anti-depressant; Cost variation; Amitriptyline; Fluoxetine; Sertraline
Abbreviations: DPCO: Drug Price Control Odder; NPPA: National Pharmaceutical Pricing Authority

Cost Variation Analysis of Various Brands of Anti-Depressants Agents Currently Available in Indian Markets
Manpreet, Shamsher Singh1, GD Gupta1 and Khadga Raj Aran1,2*
1ISF College of Pharmacy (An Autonomous College), Moga, Punjab - 142001, India
2Research Scholar, I. K. Gujral Punjab Technical University, Jalandhar, India
*Address for Correspondence: Khadga Raj Aran, Research Scholar, Neuroscience Division, ISF College of Pharmacy (An Autonomous College), Moga, Punjab 142001, India, Email: [email protected]
Depression is a mental disorder that affects the mind. It is estimated that 59% of adults suffer from melancholy worldwide [1,2]. Depression is characterized by persistent sadness and a loss of interest or enjoyment in formerly rewarding or pleasurable activities [3,4]. Symptoms of major depression include a depressed mood, loss of interest and delight, low energy, and feelings of remorse, among others. It may be a unipolar or bipolar cyclic disorder, characterized by manic and depressive cycles [5,6]. The mood change may have a psychotic basis with delusional overthinking or occur in isolation and induce anxiety that may lead to depression [7-9]. Many antidepressant classes have become available in India throughout the years; some of these classes survived the test of time and are still in use, while others are no longer marketed or are no longer a favorite with physicians [10,11]. In general, antidepressant research in India has followed Western tendencies; nevertheless, some of the antidepressant medications that have been released haven’t undergone as comprehensive of an evaluation as others [12-14]. The study of prescription patterns can assist in identifying prevalent practices of medication use in the real world. In India, the antidepressant prescription pattern has been investigated. The majority of previous Indian studies examining antidepressant prescription patterns only examined the pattern of antidepressant use in unipolar depression and the initial prescription administered to patients [15-17]. According to the World Health Organization (WHO), depression is a mood disorder and common mental disorder that affects individuals of all ages, races, ethnicities, and genders. Some varieties of depression, such as dysthymic disorder and major depressive disorder (MDD), which is the most studied form of depression, have been studied extensively [18-20].
Pathophysiology
Despite the fact that neurophysiology and neuropsychiatry research is advancing our understanding of the pathophysiology of depression, there is still much to learn [21,22]. Partially because depression is a heterogeneous disorder with complex phenomena and multiple potential etiologies, the precise mechanism by which depression develops is incomplete [23-25]. The goal is to obtain a comprehensive understanding of the pathophysiology of a disease. In the case of depression, insufficient knowledge of pathogenesis helps to explain why certain interventions fail to produce the desired effect [26-28]. The biogenic amine hypothesis, disruption of the Hypothalamic-Pituitary-Adrenal (HPA) axis, and genetic and environmental variables are now accepted processes that try to explain the pathophysiology of depression [29]. The following are some of the medications used to treat depression [30]. Drugs used to treat depression include reversible MOA (monoamine oxidase) inhibitors such as moclobemide and clorgyline, selective serotonin reuptake inhibitors (fluoxetine, fluvoxamine, and paroxetine), and atypical antidepressants (trazodone, bupropion, and amoxapine) [31].
The treatment of depression is a difficult task, as is the selection of a suitable substance to control mental disorders [32]. The cost of medications is an important aspect of health economics and plays a crucial role in care, particularly in developing nations. It is also an essential component of rational drug prescription that influences treatment adherence [33,34]. In India, the availability of antidepressants in a variety of dosage forms with varying labels and a significant price disparity generates a great deal of difficulty for physicians in choosing the least expensive medication for their patients [35]. Due to the increasing cost variation of antidepressant medications, there is a decline in patient compliance, which in turn diminishes their quality of life and increases their economic burden [36]. The awareness of the cost variation of antidepressant medications can be applied to more cost-effective treatment regimens to increase patient compliance and reduce therapy failure rates [37]. Due to the paucity of literature on the cost-effective analysis of antidepressant drugs, there is a need for cost analysis of available formulations of antidepressant drugs in the practice of medicine; thus, this study was designed. This study aims to analyse the cost variation of various brands of anti-depressants drugs currently available in the Indian pharmaceutical market [38].
This was an analytical study (current index) that analyzed the maximum and minimum prices of antidepressant medications in all available strengths and dosage forms manufactured by various companies in India. The study included these drug formulations with identical potency, dosage, and number [39]. These medications are produced by various Indian pharmaceutical companies, and fixed-dose combinations were not considered. Using the percentage cost difference between the most expensive and least expensive antidepressant brands, further analysis was conducted [40]. We can determine how frequently the most expensive brand in each category is more expensive than the least expensive brand from this. Percentage cost variation was calculated as follows [41].
Cost variation (%) = (Maximum cost – Minimum cost) / Minimum Cost × 100%
The costs of anti-depressant medications produced by various pharmaceutical companies were examined. The current investigation revealed a significant range in the highest and least cost of antidepressant medications produced by various Indian companies. The pricing of various brands of the same antidepressant agents varies substantially in the Indian market, as indicated in Table 1. The highest % cost variation was found for Amitriptyline 25 mg (195%), Fluoxetine 20 mg (95%), Sertraline 50 mg (83%), and the lowest % cost variation was for Fluvoxamine 20 mg (13.8%), Duloxetine 20 mg (16%) and Escitalopram 10 mg (38%) Figure 1.
| Table 1: Shows the price variation of anti-depression drugs. In this group, Amitriptyline showed a maximum price variation of 195%, while Fluvoxamine showed a minimum price variation of 13.8%. | |||||
| Drugs | Composition | Company | Packing | MRP (Maximum Rate and Minimum Rate) | Ratio |
| Amitriptyline | 25 mg | Indas Pharma | 10 | Max:59 | 195% |
| Min:20 | |||||
| Duloxetine | 20 mg | Sun Pharmaceuticals Industries | 10 | Max:116 MIN:100 | 16% |
| Escitalopram | 10 mg | Indas Pharma Indus. | 10 | Max:125 | 38.80% |
| Min:90 | |||||
| Fluvoxamine | 50 mg | Sun Pharma Industries | 10 | Max:156 MIN:137 | 13.80% |
| Fluvoxetine | 20 mg | Icon Life Industries | 10 | Max:80 | 95% |
| Min:41 | |||||
| Sertaline | 50 mg | Torlent Pharma LTD | 10 | Max:147 | 83% |
| Min:80 | |||||
| Desvenlafaxine | 50 mg | Sun Pharma Industries LTD | 10 | Max:153 MIN:144 | 60% |
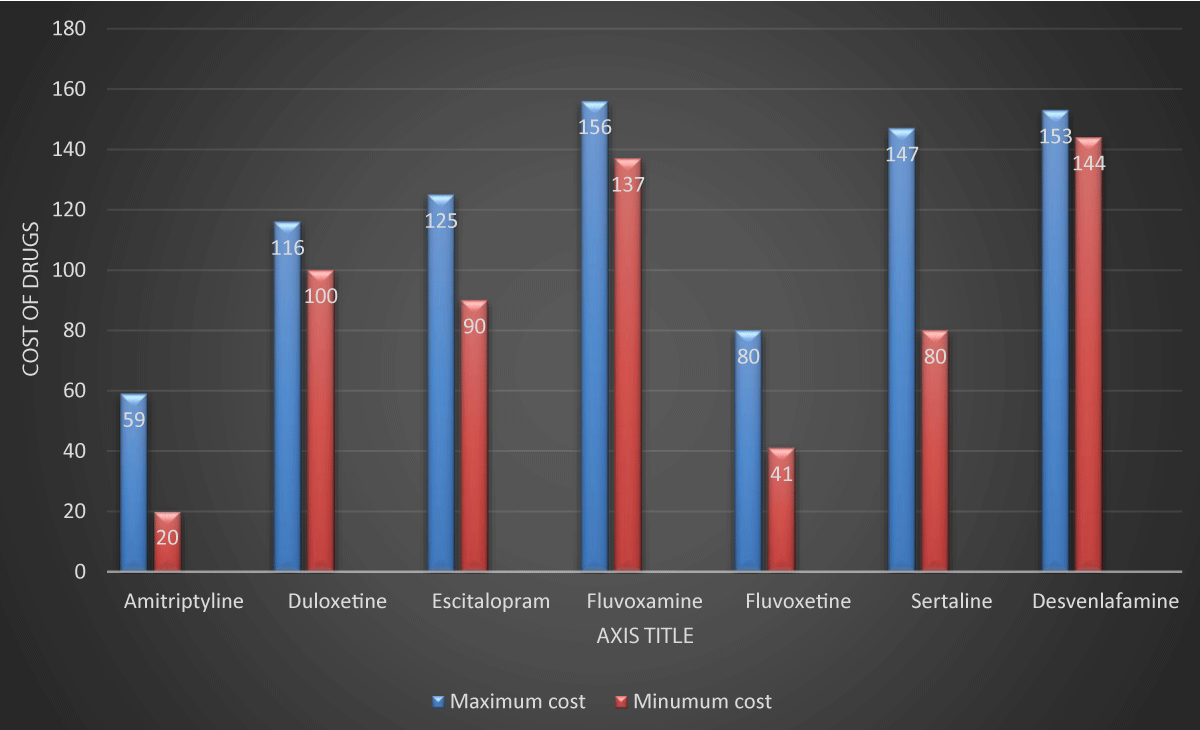
Figure 1: Cost difference [min and max] commonly used anti-depressants drugs used as single drug therapy. The maximum and minimum costs of drugs have been mentioned in the figure.
The study mentioned above shows a significant range in the maximum and cheapest cost of antidepressant medications. With the majority of anti-depressant medications, the cost variance as a percentage was greater than 100% Amitriptyline, and the price of various brands of the same anti-depressant medications on the Indian market varies significantly. Medication noncompliance is the most frequent cause of medication nonadherence, and it has been demonstrated to be related to higher drug costs. It has been found that up to 90% of depressed individuals are non-compliant. When depression is not treated as prescribed, the mental condition progresses, drastically raising the expense of overall medical care. The issue could be improved if the drug price is given more importance when pharmaceuticals are in drug price order. The National Pharmaceutical Pricing Authority (NPPA) and the Drug Price Order DPCO) are effective tools for regulating drug costs [42]. As per a previous study, it was found that a significant range in the costs of different antidepressant formulations. Their research found that only Escitalopram price fluctuation was investigated. In order to examine the price variance of antidepressant drugs accessible on the Indian market, research was created. The top 25 medications in our hospital system are listed here. In developing nations, patients are responsible for covering their own medical expenses [43,44]. In India, patients foot more than 80% of the bill for healthcare. The government should adopt a policy that allows for the reasonable and accessible pricing of branded and generic medications. The study’s weakness is that the price variations in the parenteral antidepressant formulation were not examined [45]. The analysis excluded certain medications used to treat depression. Another study was performed by Tripathi et al., in the year 2018 and they found there are 15 medications with 63 formulations under 1173 brands produced by various pharmaceutical companies. According to the results of this study, there are many different brands of antidepressant medications on the market, and the prices of these medications vary greatly. As a result of their analysis, we came to the conclusion that the antidepressant medicine market in India has a wide range of prices and brand names. By prescribing medications with generic names rather than specific names, this variation could be reduced. Additionally, choosing medicine brands with modest maximum dosages will be appropriate financially. Among all the antidepressant drugs, the highest cost ratio and percentage cost variation were found for the fluvoxamine 100 mg which is 1:12. 274 and 1127. 495 followed by amitriptyline 50 mg [1:5.558 and 455.813], which is similar to our study.
The above study depicts more variation in the various prices of different brands of the same anti-depressants drugs presently available in the Indian market. Increased adherence to the therapy can be ensured by decreasing the price of therapy by changes in government policies and regulations and creating awareness among curing physicians for switching to cost-effective therapy and thus help in rational prescribing.
Prescribing medications should be given greater emphasis among practitioners and also spreading awareness that cheaper medicines are not inferior to costlier branded counterparts. Financial constraints are a reality in almost all aspects of medical doctors have to consider the price of medications to their patients. Patients are adversely affected by raising medication costs given the increasing prescribing, taking into account prescription costs.
We are thankful to Praveen Garg, Chairman, ISFCP, Moga, Punjab for providing the necessary facilities and Prof GD Gupta and Dr. Shamsher Singh for designing, analysing, and completing the study.
Availability of data and materials: All data generated or analyzed were included in this published article.
Authors contributions: Author’s contributions this study are: KRA: main author, design, methodology and writing, M: coordination and design.
- Goldman LS, Nielsen NH, Champion HC. Awareness, diagnosis, and treatment of depression. J Gen Intern Med. 1999 Sep;14(9):569-80. doi: 10.1046/j.1525-1497.1999.03478.x. PMID: 10491249; PMCID: PMC1496741.
- Lewinsohn PM, Rohde P, Seeley JR, Fischer SA. Age-cohort changes in the lifetime occurrence of depression and other mental disorders. J Abnorm Psychol. 1993 Feb;102(1):110-20. doi: 10.1037//0021-843x.102.1.110. PMID: 8436687.
- Rottenberg J, Kasch KL, Gross JJ, Gotlib IH. Sadness and amusement reactivity differentially predict concurrent and prospective functioning in major depressive disorder. Emotion. 2002 Jun;2(2):135-46. doi: 10.1037/1528-3542.2.2.135. PMID: 12899187.
- Der-Avakian A, Mazei-Robison MS, Kesby JP, Nestler EJ, Markou A. Enduring deficits in brain reward function after chronic social defeat in rats: susceptibility, resilience, and antidepressant response. Biol Psychiatry. 2014 Oct 1;76(7):542-9. doi: 10.1016/j.biopsych.2014.01.013. Epub 2014 Jan 31. PMID: 24576687; PMCID: PMC4117827.
- Uher R, Payne JL, Pavlova B, Perlis RH. Major depressive disorder in DSM-5: implications for clinical practice and research of changes from DSM-IV. Depress Anxiety. 2014 Jun;31(6):459-71. doi: 10.1002/da.22217. Epub 2013 Nov 22. PMID: 24272961.
- Pfennig A, Ritter PS, Höfler M, Lieb R, Bauer M, Wittchen HU, Beesdo-Baum K. Symptom characteristics of depressive episodes prior to the onset of mania or hypomania. Acta Psychiatr Scand. 2016 Mar;133(3):196-204. doi: 10.1111/acps.12469. Epub 2015 Aug 7. PMID: 26252885.
- Černis E, Freeman D, Ehlers A. Describing the indescribable: A qualitative study of dissociative experiences in psychosis. PLoS One. 2020 Feb 19;15(2):e0229091. doi: 10.1371/journal.pone.0229091. PMID: 32074139; PMCID: PMC7029850.
- Aung SK, Fay H, Hobbs RF 3rd. Traditional Chinese Medicine as a Basis for Treating Psychiatric Disorders: A Review of Theory with Illustrative Cases. Med Acupunct. 2013 Dec 1;25(6):398-406. doi: 10.1089/acu.2013.1007. PMID: 24761185; PMCID: PMC3870484.
- Kaiser BN, Haroz EE, Kohrt BA, Bolton PA, Bass JK, Hinton DE. "Thinking too much": A systematic review of a common idiom of distress. Soc Sci Med. 2015 Dec;147:170-83. doi: 10.1016/j.socscimed.2015.10.044. Epub 2015 Oct 21. PMID: 26584235; PMCID: PMC4689615.
- Siddiqui RA, Shende TR. Prescription pattern of antidepressant drugs in a tertiary care centre of central India. J Cont Med A Dent. 2014; 2(2):14-6.
- Gilani AH, Rahman AU. Trends in ethnopharmocology. J Ethnopharmacol. 2005 Aug 22;100(1-2):43-49. doi: 10.1016/j.jep.2005.06.001. PMID: 16127805.
- Avasthi A, Grover S, Aggarwal M. Research on antidepressants in India. Indian J Psychiatry. 2010 Jan;52(Suppl 1):S341-54. doi: 10.4103/0019-5545.69263. PMID: 21836704; PMCID: PMC3146188.
- Grover S, Dutt A, Avasthi A. An overview of Indian research in depression. Indian J Psychiatry. 2010 Jan;52(Suppl 1):S178-88. doi: 10.4103/0019-5545.69231. PMID: 21836676; PMCID: PMC3146226.
- Tunkel DE, Bauer CA, Sun GH, Rosenfeld RM, Chandrasekhar SS, Cunningham ER Jr, Archer SM, Blakley BW, Carter JM, Granieri EC, Henry JA, Hollingsworth D, Khan FA, Mitchell S, Monfared A, Newman CW, Omole FS, Phillips CD, Robinson SK, Taw MB, Tyler RS, Waguespack R, Whamond EJ. Clinical practice guideline: tinnitus. Otolaryngol Head Neck Surg. 2014 Oct;151(2 Suppl):S1-S40. doi: 10.1177/0194599814545325. PMID: 25273878.
- Pant P, Dhamija P, Ahmad Y, Srivastava P. Off-label use of antipsychotics and antidepressants-a double edged sword–obliges a close monitoring. Authorea Preprints. 2020 May 26.
- Tripathi A, Avasthi A, Desousa A, Bhagabati D, Shah N, Kallivayalil RA, Grover S, Trivedi JK, Shinfuku N. Prescription pattern of antidepressants in five tertiary care psychiatric centres of India. Indian J Med Res. 2016 Apr;143(4):507-13. doi: 10.4103/0971-5916.184289. PMID: 27377509; PMCID: PMC4928559.
- Baldessarini RJ, Leahy L, Arcona S, Gause D, Zhang W, Hennen J. Patterns of psychotropic drug prescription for U.S. patients with diagnoses of bipolar disorders. Psychiatr Serv. 2007 Jan;58(1):85-91. doi: 10.1176/ps.2007.58.1.85. PMID: 17215417.
- Hidaka BH. Depression as a disease of modernity: explanations for increasing prevalence. J Affect Disord. 2012 Nov;140(3):205-14. doi: 10.1016/j.jad.2011.12.036. Epub 2012 Jan 12. PMID: 22244375; PMCID: PMC3330161.
- Ghaemi SN, Hsu DJ, Thase ME, Wisniewski SR, Nierenberg AA, Miyahara S, Sachs G. Pharmacological Treatment Patterns at Study Entry for the First 500 STEP-BD Participants. Psychiatr Serv. 2006 May;57(5):660-5. doi: 10.1176/ps.2006.57.5.660. PMID: 16675760.
- Lam MK, Lam LT, Butler-Henderson K, King J, Clark T, Slocombe P, Dimarco K, Cockshaw W. Prescribing behavior of antidepressants for depressive disorders: A systematic review. Front Psychiatry. 2022 Sep 9;13:918040. doi: 10.3389/fpsyt.2022.918040. PMID: 36159914; PMCID: PMC9501861.
- Chen L, Chung SW, Hoy KE, Fitzgerald PB. Is theta burst stimulation ready as a clinical treatment for depression? Expert Rev Neurother. 2019 Nov;19(11):1089-1102. doi: 10.1080/14737175.2019.1641084. Epub 2019 Jul 11. PMID: 31282224.
- Blackburn TP. Depressive disorders: Treatment failures and poor prognosis over the last 50 years. Pharmacol Res Perspect. 2019 May 3;7(3):e00472. doi: 10.1002/prp2.472. PMID: 31065377; PMCID: PMC6498411.
- Watt DF, Panksepp J. Depression: An evolutionarily conserved mechanism to terminate separation distress? A review of aminergic, peptidergic, and neural network perspectives. Neuropsychoanalysis. 2009 Jan 1;11(1):7-51.
- Jesulola E, Micalos P, Baguley IJ. Understanding the pathophysiology of depression: From monoamines to the neurogenesis hypothesis model - are we there yet? Behav Brain Res. 2018 Apr 2;341:79-90. doi: 10.1016/j.bbr.2017.12.025. Epub 2017 Dec 25. PMID: 29284108.
- Bogdan R, Nikolova YS, Pizzagalli DA. Neurogenetics of depression: a focus on reward processing and stress sensitivity. Neurobiol Dis. 2013 Apr;52:12-23. doi: 10.1016/j.nbd.2012.05.007. Epub 2012 Jun 1. PMID: 22659304; PMCID: PMC3570616.
- Huberty TJ. Anxiety and depression in children and adolescents: Assessment, intervention, and prevention. Springer Science & Business Media; 2012 Apr 24.
- Miller WR. Motivational interviewing with problem drinkers. Behavioural and Cognitive Psychotherapy. 1983 Apr; 11(2):147-72.
- Nordentoft M. Prevention of suicide and attempted suicide in Denmark. Epidemiological studies of suicide and intervention studies in selected risk groups. Dan Med Bull. 2007 Nov;54(4):306-69. PMID: 18208680.
- Mease P. Fibromyalgia syndrome: review of clinical presentation, pathogenesis, outcome measures, and treatment. J Rheumatol Suppl. 2005 Aug;75:6-21. Erratum in: J Rheumatol Suppl. 2005 Oct;32(10):2063. PMID: 16078356.
- Evans MD, Hollon SD, DeRubeis RJ, Piasecki JM, Grove WM, Garvey MJ, Tuason VB. Differential relapse following cognitive therapy and pharmacotherapy for depression. Arch Gen Psychiatry. 1992 Oct;49(10):802-8. doi: 10.1001/archpsyc.1992.01820100046009. PMID: 1417433.
- Grimwood S, Hartig PR. Target site occupancy: emerging generalizations from clinical and preclinical studies. Pharmacol Ther. 2009 Jun;122(3):281-301. doi: 10.1016/j.pharmthera.2009.03.002. Epub 2009 Mar 21. PMID: 19306894.
- Seligman L, Reichenberg LW. Selecting effective treatments: A comprehensive, systematic guide to treating mental disorders. John Wiley & Sons; 2011 Oct 19.
- Rathod S, Pinninti N, Irfan M, Gorczynski P, Rathod P, Gega L, Naeem F. Mental Health Service Provision in Low- and Middle-Income Countries. Health Serv Insights. 2017 Mar 28;10:1178632917694350. doi: 10.1177/1178632917694350. PMID: 28469456; PMCID: PMC5398308.
- Ofori-Asenso R, Agyeman AA. Irrational Use of Medicines-A Summary of Key Concepts. Pharmacy (Basel). 2016 Oct 28;4(4):35. doi: 10.3390/pharmacy4040035. PMID: 28970408; PMCID: PMC5419375.
- Rudrapal M, Khairnar SJ, Jadhav AG. Drug repurposing (DR): an emerging approach in drug discovery. Drug Repurposing-Hypothesis, Molecular Aspects and Therapeutic Applications. 2020 Jul 13; 10.
- Reich M, Lesur A, Perdrizet-Chevallier C. Depression, quality of life and breast cancer: a review of the literature. Breast Cancer Res Treat. 2008 Jul;110(1):9-17. doi: 10.1007/s10549-007-9706-5. Epub 2007 Aug 3. PMID: 17674188.
- Kuyken W, Byford S, Byng R, Dalgleish T, Lewis G, Taylor R, Watkins ER, Hayes R, Lanham P, Kessler D, Morant N, Evans A. Study protocol for a randomized controlled trial comparing mindfulness-based cognitive therapy with maintenance anti-depressant treatment in the prevention of depressive relapse/recurrence: the PREVENT trial. Trials. 2010 Oct 20;11:99. doi: 10.1186/1745-6215-11-99. PMID: 20961444; PMCID: PMC2972263.
- Fullagar S, O'Brien W. Problematizing the neurochemical subject of anti-depressant treatment: the limits of biomedical responses to women's emotional distress. Health (London). 2013 Jan;17(1):57-74. doi: 10.1177/1363459312447255. Epub 2012 Jun 6. PMID: 22674747.
- Yin N. Pharmaceuticals, incremental innovation and market exclusivity. Toulouse School. 2012 Dec 17.
- Kumar N, Abbas A, Ahmad A, Choudhary R, Ganguly A, Dixit RK. Cost comparison of commonly used antidepressant drugs with drug price control order in India.
- Ray A, Najmi A, Khandelwal G, Sadasivam B. A Cost Variation Analysis of Drugs Available in the Indian Market for the Management of Thromboembolic Disorders. Cureus. 2020 May 5;12(5):e7964. doi: 10.7759/cureus.7964. PMID: 32523821; PMCID: PMC7273361.
- Kumar R, Joshi MM, Palod RJ, Dharmagadda S. Does India need a new pharmaceutical policy? Examining the implications of the drug price control order. Int J Health Plann Manage. 2022 Nov;37(6):3028-3038. doi: 10.1002/hpm.3554. Epub 2022 Aug 18. PMID: 35983617.
- Wetherell JL, Petkus AJ, White KS, Nguyen H, Kornblith S, Andreescu C, Zisook S, Lenze EJ. Antidepressant medication augmented with cognitive-behavioral therapy for generalized anxiety disorder in older adults. Am J Psychiatry. 2013 Jul;170(7):782-9. doi: 10.1176/appi.ajp.2013.12081104. PMID: 23680817; PMCID: PMC4090227.
- Kamran S, Saqlain M, Khan Z, Mahmood S, Ali H, Ahmad N, Shah KU. Cost analysis of registered brands of oral antidepressant drugs in Pakistan: a descriptive analysis. Expert Rev Pharmacoecon Outcomes Res. 2020 Oct;20(5):473-479. doi: 10.1080/14737167.2019.1666001. Epub 2019 Sep 13. PMID: 31498710.
- McDonnell A, Pisani E, Singhvi S, Chalkidou K, Yadav P. A path to resiliency: mitigating the impacts of COVID-19 on essential medicines supply chains. CGD Policy Paper. 2021 Jun 4; 213.
- Tripathi RK, Singh S. Cost variation analysis among different antidepressant drugs used to treat major depressive disorder. Journal of Pharmaceutical and Biological Sciences. 2019 Apr 1; 6(2):51.