
More Information
Submitted: July 19, 2023 | Approved: August 29, 2023 | Published: August 30, 2023
How to cite this article: Mihaita E, Mitrache G, Stoica M, Tonis RMB. The Dynamics of Eating Behavior Disorders and the Level of General Psychological Adaptation in Bodybuilding and Fitness Athletes. J Neurosci Neurol Disord. 2023; 7: 065-089.
DOI: 10.29328/journal.jnnd.1001081
Copyright License: © 2023 Mihaita E, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Psychological traits; Psychological scales; Threshold; Bodybuilding; Eating disorders

The Dynamics of Eating Behavior Disorders and the Level of General Psychological Adaptation in Bodybuilding and Fitness Athletes
Elena Mihaita*, Georgeta Mitrache, Marius Stoica and Rocsana Manea Bucea Tonis
National University of Physical Education and Sports, Doctoral School, Bucharest, Romania
*Address for Correspondence: Elena Mihaita, National University of Physical Education and Sports, Doctoral School, Bucharest, Romania, Email: [email protected]
Knowing the psychological traits and clinically relevant symptoms for the development and maintenance of Eating Behavior Disorders (EDD) in bodybuilding and fitness athletes is a necessity for early intervention and the elimination of stressors that contribute to improving sports performance and quality of life.
The aim of the study: To know the dynamics of EDD and the level of general psychological adaptation in athletes who practice bodybuilding and fitness according to sports gender and age.
By applying the Inventory of Eating Disorders, EDI-III on 30 participants, bodybuilding and fitness practitioners, aged between 19 and 53, of which 21 are male and 9 are female, psychological traits were investigated relevant (low self-esteem, perfectionism, asceticism, fear of maturity, interpersonal, emotional problems, exaggerated control, and others) in order to know the level of distress and the presence of clinically relevant symptoms for the development and maintenance of EDD (the desire to being thin, bulimia, body dissatisfaction)
We concluded that most of the athletes fall within the limits of the threshold values established for the evaluated scales, 30% of the athletes (3 female athletes and 6 male athletes), obtained scores rated above the threshold on at least one of the clinical scales, which means that the risk of EDD is present in some athletes. The average of the investigated psychological scales calculated for the rated scores to establish the level of general psychological adaptation does not exceed the specified threshold for each investigated dimension separately, except for the asceticism, interpersonal problems, and exaggerated control scales. Female athletes have greater psychological balance than male athletes and lower risk of ED than male athletes, important aspects of personality and mental health in psychological training as a screening tool in the process of optimizing the effectiveness of bodybuilding and fitness training.
The essential characteristic of man is to present himself as an individuality, a unique result of the convergence of a multitude of biological, psychological, social, and cultural factors that give him uniqueness both in the mental and behavioral spheres [1].
Considering one of the many definitions of personality as “the dynamic organization within the individual of those psychophysical systems that determine his characteristic thinking and behavior” Golu [2] and the fact that it is manifested, revealed in what the person thinks, feels, and does, knowing its dimensions can lead to novel solutions applied to athletes who practice bodybuilding and fitness.
The constellation of mental and physical states that facilitate the achievement of superior results in competitions inevitably depends on the gender and age of the athletes and on the sport practiced / branch (in addition to the inter-individual differences related to the unique and original personality of each person) [3].
Bodybuilding and fitness represent an activity that is located at the intersection of the physical, mental, and social, having formative effects, such as team spirit, cooperation, the need to become sociable, civilized behavior, fair play, and discipline.
Practicing bodybuilding and fitness requires organizing life by adopting a healthy lifestyle due to training routines, nutrition (hyperprotein to promote muscle mass growth, hypoglycemic to reduce adipose build-up), rest, physical fatigue and mental stress negatively affecting effort parameters and muscle strength level.
By increasing the number of people who adhere to the concept of sport for all, choosing a form of exercise as a way of spending their free time, in this case “going to the gym” [4], the triad of the need for exercise-healthy nutrition-rest for the well-being is outlined on a physical level by increasing muscle tone and a body weight index in optimal parameters and on a psychological level, reducing the level of stress through nervous discharge that can be achieved with lifting/pushing weights, followed by mental relaxation.
Bodybuilding or physical culture is a discipline that, through training with weights, overloads (resistance training), and a specific diet, has as its final objective the change of body composition with the increase of muscle mass and the reduction of body fat, where the goals are aesthetic but also competitive.
Bodybuilding is one of the sports activities that identify with masculinity and includes several characteristics such as being muscular, having an enlarged physical appearance, and being strong and competent. In this regard, research has been conducted on muscle dysmorphic disorder, narcissistic personality traits, and body image disorder in male bodybuilders. An interesting study involving 63 bodybuilders and 65 sedentary men [5] indicates that as bodybuilders’ desire to become more muscular and strong increases, the degree of positive body perception decreases and there is a relationship between bodybuilders’ physical dissatisfaction and their physical appearance. As a result of this finding, it can be said that individuals who become bodybuilders turn to bodybuilding as a result of this dissatisfaction. Additionally, it can be argued that bodybuilders’ body dissatisfaction is a factor that may be associated with the development of Muscle Dysmorphia (MD) and that they turn to bodybuilding to have the body they want.
The authors of the study Pursuit of the muscular ideal: Physical and psychological consequences and putative risk factors [6] believe that developing a lean muscular figure for athletic and/or appearance purposes has become a central problem for men. Concern has been raised because the desire to develop such a body build can lead to the adoption of numerous health-threatening behaviors.
Self-esteem is not the first reason men become competitive amateur bodybuilders, emulation was the largest category stated for starting bodybuilding (n = 118), followed by previous participation in sports (n = 107), self-esteem (n = 107) = 50), health (n = 36) and other (n = 28), concluded [7] studying the reasons why men become competitive amateur bodybuilders.
The results of the study Personality Factors in Exercise Addiction: A Pilot Study Exploring the Role of Narcissism, Extraversion, and Agreeableness [8] indicate a low incidence of people who were classified as being at risk of exercise addiction (7% ), but a high incidence of symptomatic individuals (75%). The results suggested that extraversion and narcissism may be underlying factors in exercise addiction with no effect on agreeableness. Exercise engagement and intensity were also related to exercise addiction. Further research examining the relationship between personality types and exercise addiction may be helpful in identifying individuals at risk for developing exercise addiction.
Research topics such as self-enhancement, attention and self-control, knowledge and experience development, well-being, and life have been integrated into the concept of “extraordinary self” based on the fact in the studies “Self-enhancement: bodybuilders make sense of the experiences with which they improve themselves”. appearance and performance [9], whereby participants realized a potential “exit point” that undermined the use of Appearance and Performance-Enhancing Drugs (APEDs) emerged from a tension between such “extraordinary selves” and “ the ordinary self’ whereby they perceived APEDs as preventing them from living a normal, balanced life outside of the context of bodybuilding.
Hegemonic masculinity takes different forms in different fields of interaction, acting as a form of cultural capital: gender capital. Inherent in this discussion is the cultural contradictions evident among individuals struggling to physically or ideologically embody gender capital. Individuals may attempt to embody hegemonic idealizations, but bodies are not only inscribed with gender, the inscriptions are read and read differently by different social actors and in different contexts. The capacity of gendered capital to remain elusive is precisely what allows gendered practices and projects such as bodybuilding to retain passionate participation [10].
Contemporary life has turned the body into an object of increasing interest. The real emphasis of our culture is not on the body as the “material substrate” of the person, but on the body as the ideal appearance and the very repository of social rules and norms.
In the study “The Contemporary Construction of a Perfect Body Image: Bodybuilding, Exercise Addiction and Eating Disorders” [11], the author emphasizes the dynamic similarities between anorexic and addictive exercise behaviors and shows that the ultimate consequences of strong manipulation of our real body can be a pathological behavior, thus many bodybuilders and anorexics can be seen as “victims” of the extreme control of their bodies and the contemporary construction of an ideal body image.
Body image, binge eating, and bulimia nervosa in male bodybuilders (Goldfield, et al. 2006) is an ongoing concern for the general population, given the rate of obesity worldwide, and for athletes in particular in the run-up to competitions to fit within the categories and reduce the fat layer to the minimum necessary for the normal functioning of the body. Men with Bulimia Nervosa (MBN), Competitive Male Bodybuilders (CMBB), and Recreational Male Bodybuilders (RMBB) were compared on a wide range of eating attitudes and behaviors and psychological characteristics to further determine similarities and differences between these groups.
High rates of weight and shape preoccupation, extreme body modification practices, binge eating, and Bulimia Nervosa (BN) have been reported among Male Bodybuilders (MBB), particularly those who have competed. CMBB reported higher rates of binge eating, BN, and AAS compared to RMBB, but showed less overall and eating-related psychopathology compared to MBN. Few psychological differences were found between CMBB and RMBB. MBB, especially competitors, and MBN appear to share many nutritional characteristics but few general psychological ones. The study author concluded that longitudinal research is needed to determine whether men with a history of disordered eating or BN gravitate disproportionately toward competitive bodybuilding and/or whether competitive bodybuilding promotes disordered eating, BN, and AAS use. The relationship between the risk of muscle dysmorphia and psychopathological symptoms in an Italian sample of male bodybuilders was also investigated in the study “Muscle dysmorphia and psychopathology: findings from an Italian sample of male bodybuilders” (Longobardi, et al. 2017), during which participants completed the Muscle Dysmorphic Disorder Inventory (MDDI), Symptom Checklist-90-R (SCL-90-R), Dissociative Experiences Scale. (DES-II) and provide other socio-demographic data. Bodybuilders at risk for muscle dysmorphia exhibit greater global psychopathology and show higher scores on all dimensions of the SCL-90-R compared to bodybuilders not at risk for muscle dysmorphia. In addition, the risk of muscle dysmorphia is positively associated with dissociative symptoms.
Dissatisfaction with the image, especially in aspects related to body weight, is predominantly present in women, the level of dissatisfaction can lead to the rejection of its image which is a process of self-acceptance present in the social groups of the population, a study in this sense was initiated to analyze the level of body image satisfaction in female bodybuilders practicing different levels of physical activity (Franco, et al. 2021). It was found that there was no difference between the groups in terms of current figures and dissatisfaction. There was a significant difference when comparing the current bodybuilding and bodybuilding figure options to the options of undergraduate physical education students.
The drive for muscularity and muscle dysmorphic tendencies were found to be prevalent in Pakistani culture, concludes a bodybuilding study that assessed the relationship between the desire for muscularity and muscle dysmorphic tendencies in 211 subjects with an average age of 26.25 +/- 5,946 years. The cross-sectional study (Bashir, et al. 2021) was conducted in Lahore, Pakistan, from June to September 2017, and included male bodybuilders in early and middle adulthood. Data were collected using a native Drive for Muscularity inventory and the Body Dysmorphic Disorder factors of the Yale-Brown Obsessive Compulsive Scale. There was a positive relationship between the drive for muscularity and muscle dysmorphic tendencies. Of the total, 130 (62%) bodybuilders had a moderate level of desire for muscle. Unmarried bodybuilders aged 18 - 25 had a greater desire for muscle compared to married bodybuilders aged 26 and over.
The Eating Disorder Inventory (EDI) is used worldwide in research and clinical practice. The third version (EDI-3) was used by several researchers to adapt and standardize the EDI-3 at the national level and applied to representative samples of the population. The factor structure is confirmed, the internal consistency of the subscales being satisfactory, the discriminative validity good, and sensitivity and specificity, excellent [12], aspects also confirmed at the level of Romania, respectively good internal consistency, increased level of fidelity and validity [13].
Purpose of the study
Knowledge of the dynamics of psychological traits (low self-esteem, personal alienation, interpersonal insecurity, interpersonal alienation, interoceptive deficits, emotional imbalance, perfectionism, asceticism, fear of maturity) and clinically relevant symptoms for the development and maintenance of behavioral disorders food (desire to be thin, bulimia, body dissatisfaction, risk of eating disorder, ineffectiveness, interpersonal problems, emotional problems, exaggerated control, general psychological maladjustment).
Hypotheses
➣ There are respondents who show clinically relevant symptoms of eating disorders;
➣ The athletes show a good general psychological adaptation related to the investigated psychological traits
➣ There is a dynamic of psychological traits that are reflected in the differences in the perception of the athletes at the level of the investigated psychological scales.
The methods of observation, conversation, measurement, test method, and statistical methods were used in the research.
Tasks
✓ Complex evaluation of the athletes’ personality;
✓ Generation of psychological evaluation reports;
✓ Centering the results and establishing the dynamics of the investigated scales according to gender and sports age.
Application of the eating disorder inventory EDI-III.
Presentation of the applied questionnaire. Brief description of the investigated psychological scales.
Interpretation of the scores of the investigated psychological scales and the use of T-scores.
The Eating Disorder Inventory-3 (EDI-3) is an instrument with a high level of reliability and validity in the assessment of clinically relevant symptoms of eating disorders.
The eating behavior disorder inventory EDI-III [14] is intended for administration in the general (non-clinical) population, in people aged at least 18 years, being a standardized tool for self-assessment of relevant psychological traits from a clinical point of view for people showing symptoms of eating disorders. It evaluates characteristic features of this category of disorders: The desire to be thin, bulimia, and dissatisfaction with the body, as well as nine psychological constructs, important both in the emergence and in the manifestation and maintenance of eating disorders. Similar to the results obtained by the authors of this inventory, the Romanian version of the EDI-3 discriminates between people with a clear diagnosis of an eating disorder and those without such a pathology, recommending its use both as a screening tool, as well as an adjunct tool in assessing the severity of the present symptoms of eating disorder.
The rating system of EDI-3
The response options to the items in EDI-3 are ordered on a 6-point scale, with the obligatory choice of a variant, and the respondent must determine for each item if it suits them. Each item is assigned a score from 0 to 4, Always, Usually, Often, Sometimes, Rarely, or Never, so that extreme responses indicating the presence of symptomatology or pathology (either Always or Never, depending on whether the item is directly or reverse scored) are scored 4. The response immediately adjacent (Usually or Rarely), receives a score of 3, the next adjacent response (Often or Sometimes) receives a score of 2, the next (Sometimes or Often), receives a score of 1, and the next two responses in the opposite direction of a pathological manifestation receive a score of 0, the scale score being calculated by simply adding up all the scores of the respective scale items. This rating system preserves the heuristic value of the initial rating system and widens the range of scores, improving the psychometric quality of the inventory for the non-clinical population, in the case of our bodybuilding and fitness athletes.
The use of confidence intervals of T-rates allows for comparing people with each other [13].
Description and content of specific, psychological, and composite scales of EDI-III
There are 12 basic scales and six composite scales of the EDI-3, totaling 91 items, the latter being obtained by summing the T-scores of two or more scales. Three of the core scales, Desire to be Thin [DS], Bulimia [B], and Body Dissatisfaction [NC]) are labeled as Eating Disorder Risk 2 scales, and research has shown that obtaining high scores on these scales, places the respondents in the sphere of increased risk for the development of an eating behavior disorders. The other nine scales (i.e., Low Self-Esteem [SSE], Personal Alienation [AP], Interpersonal Insecurity [NI], Interpersonal Alienation [AI], Interoceptive Deficits [DI], Emotional Imbalance [DE], Asceticism [A], Fear of Maturity [FM]) assess relevant psychological constructs conceptual for the evolution and maintenance of eating behavior disorders. EDI‑3 also presents three “item clusters” that provide additional information in relation to several specific areas of interest.
Eating disorder risk scales [13]
Desire to be thin scale (DS)
Scale description: The construct “desire to be thin” has been described as one of the basic characteristics of eating disorders and has been considered an essential diagnostic criterion, according to many classification systems. The seven items of this scale assess:
a) strong desire to be thinner,
b) concern related to diets,
c) weight concern
d) intense fear of not gaining weight.
Bulimia scale (B)
Scale description: Scale B assesses the tendency to think about and engage in episodes of excessive and uncontrolled eating (compulsive eating). The eight items of this scale assess preoccupation with compulsive eating and eating in response to distress. The presence of episodes of compulsive eating is one of the defining features of BN and differentiates AN‑R (restrictive type) from AN‑AC/V (a type characterized by compulsive eating behavior/vomiting).
Body dissatisfaction scale (NC)
Scale description: The NC scale consists of 10 items that assess dissatisfaction with the shape and size of certain areas of the body, aspects that are a particular cause of concern for people with eating disorders (in other words, it is about the belly, hips, thighs, and buttocks).
Psychological scales
The SSS scale measures the primary concept of self-evaluation in negative terms. Five of the six items of the scale refer to emotionally saturated constructs, related to feelings of insecurity, inadequacy, inefficiency, and self-devaluation. The other item measures the individual’s perception of his inability to meet his own standards. Most theories believe that low self-esteem plays an important role in the emergence and maintenance of eating disorders.
Personal alienation scale (PA)
The Personal Alienation scale conceptually overlaps with the Low Self-Esteem scale, but measures a broader domain, reflecting characteristics such as a generalized sense of emotional deprivation, loneliness, and a low ability to understand one’s own self.
The seven items of the AP scale refer to contents that reflect feelings of isolation towards the rest of the people, of defeat or non-recognition of the merits by the others. The items of the AP scale also measure the respondent’s desire to be someone else, as well as a general feeling of lack of control over events in one’s life.
Interpersonal insecurity scale (NI)
The Interpersonal Insecurity scale is made up of seven items that evaluate the states of discomfort, anxiety, and reluctance in social situations. This focuses mainly on difficulties in expressing one’s thoughts and emotions to others. The content of the items in this scale also aims to evaluate the tendency of withdrawal and social isolation.
Interpersonal alienation (AI) scale
The seven items of the Interpersonal Alienation scale assess disappointment, distancing, alienation, and lack of trust in interpersonal relationships. Also, the items measure the tendency to feel trapped in relationships, as well as the impression that others do not offer enough affection and understanding.
A high score on the AI scale indicates a fundamental inability to form attachment interpersonal.
Interoceptive deficits (DI) scale
The Interoceptive Deficits scale consists of nine items that measure the state of confusion associated with the ability to recognize and respond adequately to emotional states.
Within the DI scale, two clusters were identified. First, there is a cluster called Fear of Emotions, which identifies a state of distress when emotions are too strong or out of control. Second, the cluster called Confusion about emotions highlights difficulties in the adequate recognition of emotional states. Confusion and lack of confidence about physical and emotional functioning have been repeatedly recognized as important characteristics of people with eating disorders.
Emotional imbalance scale (ED)
The Emotional Imbalance scale is composed of eight items that assess the tendency toward mood instability, impulsivity, recklessness, anger, and self-destructive behaviors. This scale contains a cluster consisting of two items. These two items refer to possible substance abuse problems: one for alcohol and one for medication. Tendencies toward poor impulse self-regulation and intolerance to changes in mood were identified among the signs of an unfavorable prognosis in eating disorders.
Perfectionism scale (P)
The Perfectionism scale contains six items that determine the degree to which a person values the achievement of great goals and particularly high standards of personal success.
The content of the items of this scale falls into two content areas. The first is “self-oriented perfectionism” and reflects rigorous personal standards of performance. The second is “socially prescribed perfectionism” and refers to performance requirements resulting from pressure exerted by parents and teachers. Research has shown that perfectionism can underlie relentless efforts to control weight, as well as unrealistic efforts in other areas.
Asceticism scale (A)
The Asceticism scale consists of seven items that assess the tendency to seek virtue through the pursuit of spiritual ideals, such as self-discipline, self-denial, self-restraint, self-sacrifice, and control of bodily needs. Ascetic motivation for weight loss continues to be an important theme in some cases. Asceticism can be expressed through food restriction as a form of purification, low weight can be considered a virtue, and fasting - an act of penance. Rejecting food and abstaining from food can be part of a more general theme of giving up physical gratifications. The concept of asceticism can have either positive connotations, of obtaining virtue through self-control, or negative connotations (for example, guilt and shame) towards pleasant.
Fear of maturity scale (FM)
The FM scale consists of eight items that assess the desire to withdraw into the atmosphere safe childhood. This construct is considered a central factor in maintaining the pathology in a subgroup of adolescent patients, whose food restriction and weight loss are functional because it provides the means to return to a puberty-specific appearance and hormonal balance. In this way, they can withdraw from the agitation and conflicts, and avoid the expectations related to development, specific to adulthood.
The fear of developing can stimulate the emergence of other fears and expectations related to role changes, which teenagers, their parents, or others do not feel prepared to face.
Composite scales
Eating Disorder Risk Composite Scale (SCRTCA) The SCRTCA score is obtained by summing the T scores on the DS, B, and NC scales. It provides a global measure of these constructs, each of the scales contributing equally to its value. The SCRTCA score can be used for screening or to obtain a single score that reflects the level of dietary concerns.
Ineffectiveness composite scale (SCI)
The score of this scale is calculated by summing the T scores on the SSS and AP scales. These two scales correlate strongly in both clinical and non-clinical populations, and their combination generally improves fidelity.
Interpersonal problems composite scale (SCPI)
The SCPI score consists of the sum of the T scores on the NI and AI scales. These two scales correlate only moderately with each other.
Emotional problems composite scale (SCPE)
The SCPE score is calculated by summing the T scores on the DI and DE scales. These two scales correlate moderately between them. The SCPE score reflects severe deficits in individuals’ way of interpreting emotional stimuli and responding to them. Those patients with eating disorders who have difficulties in understanding their own emotional states and with a tendency to react impulsively, with anger, through changes in affective mood, or through substance abuse, can raise serious problems in therapy. The difficulty with which an individual identifies and tolerates his emotional states can be an important factor in maintaining an eating behavior disorder and constitutes a central element in therapy.
Exaggerated control composite scale (SCCE)
This score is calculated by summing the T scores on the A and P scales. Together, these scales reflect the attempt to achieve perfection through self-denial and suffering. Perfectionism, accompanied by extreme self-sacrifice and control of bodily needs, finds its historical origins in the sermons of religious ascetics, who were adherents of establishing purity and spiritual goals that were often harmful to the body. The composite score can have different meanings within a diagnosis of eating disorder; usually, however, it denotes the existence of defining constructs for the patient, which are extremely resistant to change due to their association with virtue.
General psychological maladjustment composite scale (SCNPG)
The SCNPG score is formed by the sum of the T scores on all nine psychological scales of the EDI‑3.
Indicators of Response Style Three validity or response style scales (Inconsistency (IN), Rarity (R), and Negative Impression (ING)) were included in the EDI‑3 inventory. These scales were constructed to establish the likelihood so that EDI‑3 scores can be interpreted.
Response style indicators
Inconsistency scale (IN): This scale indicates the extent to which the respondent gives contradictory answers to items that have similar content. For example, an individual who circles Always in response to item 2 (“I think my belly is too big”) and at the same time circles Always to item 12 (“I think my belly is the right size”) is not consistent in the way he answers.
Rarity scale (R): This scale indicates the extent to which the respondent gives answers in the direction of severe symptomatology, to items where this fact is a rarity (in general, less than 2%) among the participants in the standardization sample.
Negative impression scale (NG): The Negative Impression scale assesses the degree to which the respondent tends to respond to items in the direction of extreme symptomatology.
Research subjects and period
The study was carried out between September 2021 and February 2022 both during the weekly training program at the gym and during the National Bodybuilding and Fitness Championship organized between 09-11.09.2021 in Sibiu.
Participation in the test was voluntary based on the informed consent of each participant, and the study follows the principles of the Declaration of Helsinki, the study was approved by the Ethics Board of the National University of Physical Education and Sport, Bucharest, Romania, no 2089/ 01.10.2020.
Most of the athletes who participated in the study had notable performances both nationally and internationally. Aspects related to the equipment of the bodybuilding and fitness rooms, the training routine of the athletes, their personality and behavior in the gym were observed, and last but not least, their physical appearance was visually evaluated.
The confirmatory study was carried out with the participation of 30 athletes practicing bodybuilding, of which 9 women and 21 men, aged between 18 and 53 years, trained regularly in different bodybuilding gyms in Bucharest and the country, to participate in competitions.
The athletes selected and who agreed to participate in the study were in different stages of preparation, this being an important aspect of the research, to capture from all sides the variations of the scores on the investigated psychological scales, depending on gender and age categories sports, respectively, small juniors aged between 18-21 years, large juniors, between 21-23 years old, seniors, aged between 24-34 for women and between 24-39 for men, and the master category which includes female sportswomen over 35 years old), and in the men’s master, athletes over 40 years old.
After entering the CASS++ application, Cognitrom Assessment System [14], the answers corresponding to the items for each sport separately, the automatic assessment report was generated containing all the information about the athlete, respectively the data identification (anonymized), the qualitative information entered, the results of the applied evaluation tests (raw scores, rated scores, graphic representations, generic interpretations). CASS, Cognitrom Assessment System, version 2017, represents a computerized psychological platform made by the Cognitrom company, in a modern, flexible, open programming language that allows versatile updates and that allows the permanent updating of both items or standards for existing tests, as well as the addition of new tests for the diagnosis of all emotional and personality disorders, tests to assess the level of stress, emotional self-regulation, etc.
From the evaluation reports generated for each respondent, the answers were extracted and the values were processed in Microsoft Excel, in tables with the initials of the athletes, age, raw scores, rated scores, thresholds, or categories for each evaluated scale.
It should be noted that the period of the research coincided with the end of the COVID-19 pandemic, a period marked by movement and socialization restrictions. The bodybuilding and fitness gyms were closed the previous year, after which the operation of the gyms was conditional on compliance with certain measures to prevent infection and the spread of the virus. With restrictions on the number of people training at the same time and high and intense efforts due to the obligation to wear a protective face mask was difficult to achieve for performance athletes, as well as during endurance training when insufficient oxygen intake through wearing a mask either in the gym with specific machines or in the open air negatively conditioned the support of intense or resistance efforts, fatigue sets in faster.
Eating Disorder Inventory EDI-III. Centralization of raw scores and rated scores related to the investigated psychological scales. Descriptive statistics and percentages.
This inventory is a self-assessment tool of psychological traits and clinically relevant symptoms for the development and maintenance of eating disorders.
Clarification: The threshold used in each of the scales below represents a critical point above which it can be considered that the person presents an increased level of manifestation of the behavior described in each case.
The eating behavior disorder inventory EDI-III was divided into several sections due to the large number of evaluated scales, respectively Section 1 illustrated the results from the specific scales, Section 2 illustrated in two other subsections the psychological scales, Section 3 illustrated the composite scales, Section 4 validity scales, as presented in the tables below, as follows:
a) Inventory of eating behavior disorders EDI -III - Specific scales for eating behavior disorders (COGNITROM, 2021, updated Copyright © 2023):
Abbreviations: Specific scales for eating behavior disorders
Desire to be thin - DAS, threshold 55.27
Bulimia – B, threshold 66.04
Body dissatisfaction - NFC, threshold 56.2
The average has values above 48 for all 3 components: The desire to be thin (DAS), Bulimia B, and Body dissatisfaction (NFC), which reflected that the evaluated athletes obtained scores below the specified threshold, so the athletes do not present a level above the pathological threshold of the behavior described in each case.
The thresholds and significance of the scales related to the average scores of the study group consisting of 9 sportswomen and 21 sportsmen, according to the individual evaluation reports generated by the application are presented below, as follows:
Scale: Desire to be thin
Interpretation: The score is below the threshold which means that there are no significant concerns for nutrition and weight; there is no intense desire to be thinner and no increased fear of gaining weight.
Interpretation: There is an increased desire to lose weight, interest in slimming belts, significant preoccupation with weight, and fear of gaining weight. Specialist clinical consultation is recommended (Figure 1).

Figure 1: Example threshold exceeded on the DAS scale.
Scale: Bulimia
Interpretation: There are no thoughts and actions specific to a compulsive eating behavior or the provocation of vomiting, to lose weight.
Interpretation: Thoughts and behaviors consistent with compulsive eating are frequently present. Most of the time, the person shows the tendency to be secretive, and to have an increased level of emotional distress (negative emotional states: sadness, guilt, worry, shame, etc.). The most frequent thoughts are about the act of throwing up to lose weight. Specialist clinical consultation is recommended (Figure 2).

Figure 2: Example threshold exceeded on the Bulimia scale.
Scale: Body Dissatisfaction
Interpretation: Does not show significant dissatisfaction with body weight and shape. A very low raw score on this scale should be interpreted with caution, as it may also reflect denial of the current clinical situation or distortion of responses.
Interpretation: The presence of an accentuated dissatisfaction with the shape and size of the body, as well as with the body weight, is noted. In addition, there may be dissatisfaction with specific areas of the body - stomach, hips, thighs, and buttocks - which are a common cause for concern (Figure 3).

Figure 3: Example threshold exceeded at NFC.
In Table 1, the averages of the investigated scales for women do not exceed the threshold quotas established for each investigated scale, above which it is considered that the athletes present specific symptoms, however, 3 athletes, of which one junior and two masters exceeded at least one threshold of the DAS and NFC scales. The bulimia scale did not result in values rated above the threshold, so we can conclude that the athletes participating in the study who practice bodybuilding and fitness do not present relevant symptoms of eating behavior disorders.
| Table 1: Female scale results - EDI-III QUESTIONNAIRE - 3 SCALES, Specific scales for eating behavior disorders/raw score/rated score/threshold. | |||||||||||||
| No. crt. | Initials | Sex | Age | Waist | Weight | DAS-rated | DAS- threshold | B- raw | B-rated | B-th | NFC-raw | NFC-rated | NFC-th |
| F/M | |||||||||||||
| 1 | MM | F | 20 | 170 | 88.2 | 71.44 | 55.27 | 8 | 63.56 | 66.04 | 21 | 61.66 | 56.02 |
| 2 | NG | F | 23 | 160 | 51.5 | 49.88 | 55.27 | 4 | 53.61 | 66.04 | 2 | 40.92 | 56.02 |
| 3 | LS | F | 33 | 164 | 58 | 45.84 | 55.27 | 3 | 51.12 | 66.04 | 4 | 43.1 | 56.02 |
| 4 | GAG | F | 38 | 162 | 61.3 | 49.88 | 55.27 | 2 | 48.63 | 66.04 | 3 | 42.01 | 56.02 |
| 5 | KP | F | 42 | 160 | 52 | 53.92 | 55.27 | 6 | 58.58 | 66.04 | 7 | 46.38 | 56.02 |
| 6 | ME | F | 44 | 163 | 54 | 43.14 | 55.27 | 0 | 43.66 | 66.04 | 1 | 39.83 | 56.02 |
| 7 | RA | F | 46 | 165 | 55.6 | 63.36 | 55.27 | 2 | 48.63 | 66.04 | 23 | 63.84 | 56.02 |
| 8 | ZAM | F | 46 | 169 | 64.1 | 62.01 | 55.27 | 1 | 46.14 | 66.04 | 7 | 46.38 | 56.02 |
| 9 | ND | F | 50 | 172 | 68.3 | 45.84 | 55.27 | 0 | 43.66 | 66.04 | 5 | 45.28 | 56.02 |
| Mean | 9F | 38 | 165 | 61.44 | 53.92 | 55.27 | 2.88 | 50.84 | 66.04 | 8.11 | 47.71 | 56.02 | |
| Median | 42 | 164 | 58 | 49.88 | 55.27 | 2 | 48.63 | 66.04 | 5 | 45.28 | 56.02 | ||
| Min | 20 | 160 | 51.5 | 43.14 | 55.27 | 0 | 43.66 | 66.04 | 1 | 39.83 | 56.02 | ||
| Max | 50 | 172 | 88.2 | 71.44 | 55.27 | 8 | 63.56 | 66.04 | 23 | 63.84 | 56.02 | ||
| Notes: Inițials = The first letters of the name and surname of the participants, Specific scales for eating disorders: Desire to be thin - DAS, threshold 55.27; Bulimia – B, threshold 66.04; Body Dissatisfaction - NFC, Threshold 56.2, M = mean,m=median, min = minimum, max = maximum, th = threshold, red numbers = threshold limit exceeded, red colored numbers represent values that exceeded the threshold value for the measured scale. | |||||||||||||
In Table 2, on the DAS scale, 4 athletes of which 3 juniors and one senior exceeded the critical threshold, and another senior only reached this threshold without exceeding it. On the bulimia scale 1 junior and 3 seniors obtained values above the threshold, while on the NFC scale only two juniors obtained values above the critical threshold, they are generally satisfied with their physical appearance. The average rated scores of the specific investigated scales were not exceeded at the group level, which means that specific symptoms of eating behavior disorders are not present.
| Table 2: Male results-EDI-III QUESTIONNAIRE - 3 SCALES-Specific scales for eating behavior disorders/raw score/rated score/threshold. | ||||||||||||||
| Nr. crt. | Inițials | Sex F/M |
Age | Waist | Weight | DAS-rated | DAS-th | B-raw | B-rated | B-th | NFC-raw | NFC-rated | NFC-th | |
| 1 | NB | M | 18 | 178 | 77.6 | 60.66 | 55.27 | 8 | 63.56 | 66.04 | 17 | 57.29 | 56.2 | |
| 2 | GA | M | 19 | 185 | 75.0 | 41.79 | 55.27 | 0 | 43.66 | 66.04 | 1 | 39.83 | 56.2 | |
| 3 | RR | M | 19 | 178 | 80.5 | 63.36 | 55.27 | 10 | 68.53 | 66.04 | 19 | 59.48 | 56.2 | |
| 4 | BV | M | 20 | 173.5 | 66.3 | 45.84 | 55.27 | 1 | 46.14 | 66.04 | 3 | 42.01 | 56.2 | |
| 5 | CA | M | 21 | 180 | 73.5 | 59.31 | 55.27 | 7 | 61.07 | 66.04 | 14 | 54.02 | 56.2 | |
| 6 | TG | M | 21 | 170 | 70.0 | 45.84 | 55.27 | 3 | 51.12 | 66.04 | 9 | 48.56 | 56.2 | |
| 7 | AC | M | 23 | 180.5 | 78.6 | 41.79 | 55.27 | 2 | 48.63 | 66.04 | 10 | 49.65 | 56.2 | |
| 8 | AA | M | 24 | 192 | 105.7 | 49.88 | 55.27 | 7 | 61.07 | 66.04 | 15 | 55.11 | 56.2 | |
| 9 | OC | M | 24 | 182 | 72.9 | 48.53 | 55.27 | 2 | 48.63 | 66.04 | 13 | 52.93 | 56.2 | |
| 10 | AR | M | 25 | 186 | 74.1 | 44.49 | 55.27 | 12 | 73.51 | 66.04 | 7 | 46.38 | 56.2 | |
| 11 | CC | M | 25 | 179 | 89.0 | 52.57 | 55.27 | 12 | 73.51 | 66.04 | 4 | 43.1 | 56.2 | |
| 12 | MT | M | 25 | 175 | 85.7 | 49.88 | 55.27 | 3 | 51.12 | 66.04 | 4 | 43.1 | 56.2 | |
| 13 | SC | M | 25 | 186 | 83.5 | 44.49 | 55.27 | 0 | 43.66 | 66.04 | 9 | 48.56 | 56.2 | |
| 14 | NN | M | 26 | 184 | 67.1 | 56.62 | 55.27 | 7 | 61.07 | 66.04 | 13 | 52.93 | 56.2 | |
| 15 | FR | M | 27 | 178 | 85.0 | 45.84 | 55.27 | 0 | 43.66 | 66.04 | 0 | 38.73 | 56.2 | |
| 16 | CV | M | 31 | 180 | 88.4 | 49.88 | 55.27 | 21 | 95.9 | 66.04 | 12 | 51.83 | 56.2 | |
| 17 | PS | M | 33 | 183.5 | 93.9 | 49.88 | 55.27 | 0 | 43.66 | 66.04 | 4 | 43.1 | 56.2 | |
| 18 | PR | M | 33 | 177 | 81.1 | 47.18 | 55.27 | 3 | 51.12 | 66.04 | 7 | 46.38 | 56.2 | |
| 19 | SC | M | 33 | 166 | 80.0 | 52.57 | 55.27 | 0 | 43.66 | 66.04 | 7 | 46.38 | 56.2 | |
| 20 | PC | M | 46 | 178 | 90.6 | 48.53 | 55.27 | 1 | 46.14 | 66.04 | 0 | 38.73 | 56.2 | |
| 21 | BC | M | 53 | 188 | 109.9 | 44.49 | 55.27 | 0 | 43.66 | 66.04 | 13 | 52.93 | 56.2 | |
| Mean | 27.19 | 179.97 | 82.3 | 49.68 | 55.27 | 4.714 | 55.38 | 66.04 | 8.61 | 48.14 | 56.2 | |||
| Median | 25 | 180 | 80.5 | 48.53 | 55.27 | 3 | 51.12 | 66.04 | 9 | 48.56 | 56.2 | |||
| Min | 18 | 166 | 66.3 | 41.79 | 55.27 | 0 | 43.66 | 66.04 | 0 | 38.73 | 56.2 | |||
| Max | 53 | 192 | 109.9 | 63.36 | 55.27 | 21 | 95.9 | 66.04 | 19 | 59.48 | 56.2 | |||
| Notes: Inițials = The first letters of the name and surname of the participants Specific scales for eating disorders: Desire to be thin - DAS, threshold 55.27; Bulimia – B, threshold 66.04; Body Dissatisfaction - NFC, Threshold 56.2, M = mean, m = median, min = minimum, max = maximum, red numbers = threshold limit exceeded, green numbers = threshold limit reached. | ||||||||||||||
In Table 3, on the Desire to be thin scale, 7 athletes obtained scores rated above the threshold, respectively 3 athletes (1 junior and 2 masters) and 4 athletes (3 juniors and one senior), all with normal anthropometric values related to height and weight, with except for a 20-year-old junior athlete with a higher weight for her height, but with a higher percentage of muscle mass. On the Bulimia scale 4 athletes, of which 1 junior and 3 seniors) obtained values above the threshold, of which 2 had a higher weight compared to their height. On the Body dissatisfaction scale, 2 sportswomen (a junior and a masters category athlete) and 2 junior athletes obtained values above the threshold.
| Table 3: The threshold, raw, and rated results for EDI-III – 3 specific scales for eating behavior disorders. | |||||||||||||
| No. crt. | Initials | Sex F/M | Age | Waist | Weight | DAS-rated | DAS-th | B-raw | B-rated | B-th | NFC-braw | NFC-rated | NFC-th |
| 1 | NB | M | 18 | 178 | 77.6 | 60.66 | 55.27 | 8 | 63.56 | 66.04 | 17 | 57.29 | 56.2 |
| 2 | GA | M | 19 | 185 | 75.0 | 41.79 | 55.27 | 0 | 43.66 | 66.04 | 1 | 39.83 | 56.2 |
| 3 | RR | M | 19 | 178 | 80.5 | 63.36 | 55.27 | 10 | 68.53 | 66.04 | 19 | 59.48 | 56.2 |
| 4 | BV | M | 20 | 173.5 | 66.3 | 45.84 | 55.27 | 1 | 46.14 | 66.04 | 3 | 42.01 | 56.2 |
| 5 | MM | F | 20 | 170 | 88.2 | 71.44 | 55.27 | 8 | 63.56 | 66.04 | 21 | 61.66 | 56.2 |
| 6 | CA | M | 21 | 180 | 73.5 | 59.31 | 55.27 | 7 | 61.07 | 66.04 | 14 | 54.02 | 56.2 |
| 7 | TG | M | 21 | 170 | 70.0 | 45.84 | 55.27 | 3 | 51.12 | 66.04 | 9 | 48.56 | 56.2 |
| 8 | AC | M | 23 | 180.5 | 78.6 | 41.79 | 55.27 | 2 | 48.63 | 66.04 | 10 | 49.65 | 56.2 |
| 9 | NG | F | 23 | 160 | 51.5 | 49.88 | 55.27 | 4 | 53.61 | 66.04 | 2 | 40.92 | 56.2 |
| 10 | AA | M | 24 | 192 | 105.7 | 49.88 | 55.27 | 7 | 61.07 | 66.04 | 15 | 55.11 | 56.2 |
| 11 | OC | M | 24 | 182 | 72.9 | 48.53 | 55.27 | 2 | 48.63 | 66.04 | 13 | 52.93 | 56.2 |
| 12 | AR | M | 25 | 186 | 74.1 | 44.49 | 55.27 | 12 | 73.51 | 66.04 | 7 | 46.38 | 56.2 |
| 13 | CC | M | 25 | 179 | 89.0 | 52.57 | 55.27 | 12 | 73.51 | 66.04 | 4 | 43.1 | 56.2 |
| 14 | MT | M | 25 | 175 | 85.7 | 49.88 | 55.27 | 3 | 51.12 | 66.04 | 4 | 43.1 | 56.2 |
| 15 | SC | M | 25 | 186 | 83.5 | 44.49 | 55.27 | 0 | 43.66 | 66.04 | 9 | 48.56 | 56.2 |
| 16 | NN | M | 26 | 184 | 67.1 | 56.62 | 55.27 | 7 | 61.07 | 66.04 | 13 | 52.93 | 56.2 |
| 17 | FR | M | 27 | 178 | 85.0 | 45.84 | 55.27 | 0 | 43.66 | 66.04 | 0 | 38.73 | 56.2 |
| 18 | CV | M | 31 | 180 | 88.4 | 49.88 | 55.27 | 21 | 95.9 | 66.04 | 12 | 51.83 | 56.2 |
| 19 | LS | F | 33 | 164 | 58.0 | 45.84 | 55.27 | 3 | 51.12 | 66.04 | 4 | 43.1 | 56.2 |
| 20 | PS | M | 33 | 183.5 | 93.9 | 49.88 | 55.27 | 0 | 43.66 | 66.04 | 4 | 43.1 | 56.2 |
| 21 | PR | M | 33 | 177 | 81.1 | 47.18 | 55.27 | 3 | 51.12 | 66.04 | 7 | 46.38 | 56.2 |
| 22 | SC | M | 33 | 166 | 80.0 | 52.57 | 55.27 | 0 | 43.66 | 66.04 | 7 | 46.38 | 56.2 |
| 23 | GAG | F | 38 | 162 | 61.3 | 49.88 | 55.27 | 2 | 48.63 | 66.04 | 3 | 42.01 | 56.2 |
| 24 | KP | F | 42 | 160 | 52.0 | 53.92 | 55.27 | 6 | 58.58 | 66.04 | 7 | 46.38 | 56.2 |
| 25 | ME | F | 44 | 163 | 54.0 | 43.14 | 55.27 | 0 | 43.66 | 66.04 | 1 | 39.83 | 56.2 |
| 26 | PC | M | 46 | 178 | 90.6 | 48.53 | 55.27 | 1 | 46.14 | 66.04 | 0 | 38.73 | 56.2 |
| 27 | RA | F | 46 | 165 | 55.6 | 63.36 | 55.27 | 2 | 48.63 | 66.04 | 23 | 63.84 | 56.2 |
| 28 | ZAM | F | 46 | 169 | 64.1 | 62.01 | 55.27 | 1 | 46.14 | 66.04 | 7 | 46.38 | 56.2 |
| 29 | ND | F | 50 | 172 | 68.3 | 45.84 | 55.27 | 0 | 43.66 | 66.04 | 5 | 45.28 | 56.2 |
| 30 | BC | M | 53 | 188 | 109.9 | 44.49 | 55.27 | 0 | 43.66 | 66.04 | 13 | 52.93 | 56.2 |
| Mean | 30.43 | 175.48 | 76.04 | 50.95 | 55.27 | 4.16 | 54.02 | 66.04 | 8.46 | 48.01 | 56.2 | ||
| Median | 25.5 | 178 | 76.3 | 49.88 | 2.5 | 49.87 | 7 | 46.38 | |||||
| Min | 18 | 160 | 51.5 | 41.79 | 0 | 43.66 | 0 | 38.73 | |||||
| Max | 53 | 192 | 109.9 | 71.44 | 21 | 95.9 | 23 | 63.84 | |||||
| Notes: Inițials = The first letters of the name and surname of the participants Specific scales for eating disorders: Desire to be thin - DAS, threshold 55.27; Bulimia – B, threshold 66.04; Body dissatisfaction - NFC, threshold 56.2, M = mean,m = median, min = minimum, max = maximum, numbers colored in red represent values that exceeded the threshold value for the measured scale, th = threshold, red numbers = threshold limit exceeded. | |||||||||||||
A junior athlete scored above the threshold on all 3 scales. 9 athletes out of 30 had at least one threshold exceeded on the scales specific to eating behavior disorders, representing a percentage of 30% of the number of participating athletes, of which 3 athletes (1 junior, two masters) and 6 athletes (3 juniors and 3 seniors).
The order of the scales according to the value of the rated score is NFC, B, and DAS, which coincides in ascending order with the number of thresholds exceeded by the athletes on the mentioned scale, with most athletes falling according to age to the junior category in no. of 4, followed by 3 for seniors and 2 for masters.
According to Table 4 and Figure 4, relative to the athletes’ gender, the average value of the score on the desire to be thin scale is higher in females than in males and then the average of the 30 athletes, while the value of bulimia is higher in males than in females and is higher than the average of the participating athletes, and the body dissatisfaction scale has an approximately equal share for both women and men.
| Table 4: Centralization of scale results EDI-III questionnaire - 3 scales specific for eating behavior disorders/gross score/rated score/threshold – Average female (F), male (M), F+M. | |||||||||||||
| No. crt. | Means | Sex F/M |
Age | Waist | Weight | DAS-rated | DAS-th | B-raw | B-rated | B-th | NFC-raw | NFC-rated | NFC-th |
| 1 | Mean | F | 38 | 165 | 61.44 | 53.92 | 55.27 | 2.88 | 50.84 | 66.04 | 8.11 | 47.71 | 56.02 |
| 2 | Mean | M | 27.19 | 179.97 | 82.3 | 49.68 | 55.27 | 4.714 | 55.38 | 66.04 | 8.61 | 48.14 | 56.2 |
| 3 | Mean | F+M | 30.43 | 175.48 | 76.04 | 50.95 | 55.27 | 4.16 | 54.02 | 66.04 | 8.46 | 48.01 | 56.2 |
| Notes: Specific scales for eating disorders: Desire to be thin - DAS, threshold 55.27; Bulimia – B, threshold 66.04; Body dissatisfaction - NFC, threshold 56.2, th = threshold. | |||||||||||||
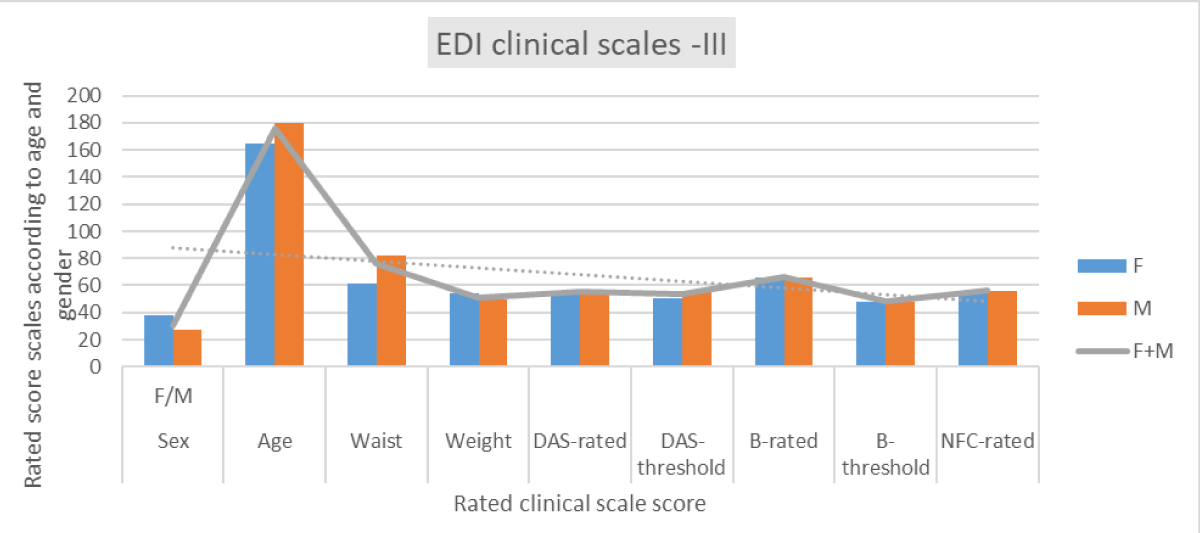
Figure 4: Graphical representation of the averages of the rated scores obtained on the clinical scales.
b) EDI -III questionnaire - PSYCHOLOGICAL SCALE, (COGNITROM, 2021, updated Copyright © 2023), critical threshold:
Low self-esteem - 60.33
Personal alienation – 61.65
Interpersonal insecurity – 52.64
Interpersonal alienation – 53.27
Interoceptive deficits – 52.97
Emotional imbalance – 58.88
Perfectionism – 54.36
Asceticism – 49.32
Fear of maturity – 51.03
The mean has values above 48 for 8 scales: SSS = Low self-esteem, AP2 = Personal alienation, NI = Interpersonal insecurity, AI = Interpersonal alienation, DI = Interoceptive deficits, DE = Emotional imbalance, P = Perfectionism, FM = Fear of maturity, the critical threshold is exceeded by the average value on the Asceticism scale, which reflected that the evaluated athletes obtained an average value below the threshold, as follows:
Scale: Low self-esteem (SSS)
Interpretation: Does not have significant problems with personal insecurity, inadequacy, ineffectiveness, or lack of self-worth.
Scale: Personal alienation (AP)
Interpretation: States may be present that refers to a general feeling of emotional emptiness and loneliness, as well as a poor understanding of one’s own person, without these being all-encompassing and significantly affecting current life.
Scale: Interpersonal insecurity (NI)
Interpretation: Suggests the existence of minimal discomfort in interpersonal or social situations, the person can have positive interpersonal relationships and good communication skills, which allow him to express his thoughts and feelings.
Scale: Interpersonal alienation (AI)
Interpretation: There is a low level of distance, alienation, and lack of trust in interpersonal relationships, the person can have positive and trusting interpersonal relationships, which give him the feeling that he is understood and loved.
Scale: Interoceptive deficits (DI)
Interpretation: There are no serious problems in identifying emotional states and responding adequately to them, there is an increased ability to deal with uncomfortable emotional experiences, positive or negative, Emotions tend, rather, to be accepted than to be critically evaluated.
Scale: Emotional imbalance (DE)
Interpretation: There are no significant problems with emotional instability, impulsivity, recklessness, anger, or self-destructive behaviors.
Scale: Perfectionism (P)
Interpretation: The presence of rigid or inadequate performance standards is not found; rather, certain more realistic expectations regarding personal success are present.
Scale: Asceticism (A)
Interpretation: The person shows a tendency to give positive connotations to activities such as self-imposed austerity, self-sacrifice, and controlling one’s own needs and does not consider that these would bring him special virtues, At the same time, he feels guilty or ashamed in the case of pleasant experiences.
Scale: Fear of maturity (FM)
Interpretation: This score indicates that the person accepts the demands of adult life, is comfortable with the challenges of growing up, and is ready to let go of the security of childhood.
In Table 5, on the low self-esteem scale, 4 athletes exceeded the threshold value, of which two juniors and 2 seniors, one being at the limit of the threshold. On the personal alienation scale, 3 junior athletes scored above the threshold, and one from the masters’ category reached the threshold without exceeding it. On the interpersonal insecurity scale, a large number of athletes obtained values above the threshold, of which 13 athletes (4 juniors, 6 seniors, 2 athletes, and one athlete from the masters category) obtained values above the threshold, and two other juniors reached the threshold quota. On the interpersonal alienation scale, 11 athletes (4 juniors and 5 seniors, one athlete and one athlete from the masters category) and two other athletes (a senior and one senior) obtained a rated value equal to the limit of the threshold value.
| Table 5: The threshold results, raw/rated score, and threshold for EDI-III – 9 psychological scales (SSS, AP, NI, and AI scales). | ||||||||||||||
| EDI -III – 9 Psychological scales | ||||||||||||||
| No. crt. | Sex | Age | SSS-raw | SSS-rated | SSS-th | AP-raw | AP-rated | AP-th | NI-raw | NI-rated | NI-th | AI-raw | AI-rated | AI-th |
| 1 | M | 18 | 9 | 62.85 | 60.33 | 13 | 71.93 | 61.65 | 16 | 67.7 | 52.64 | 15 | 69.29 | 53.27 |
| 2 | M | 19 | 0 | 40.18 | 60.33 | 0 | 38.51 | 61.65 | 3 | 43.22 | 52.64 | 0 | 34.97 | 53.27 |
| 3 | M | 19 | 6 | 55.29 | 60.33 | 17 | 82.21 | 61.65 | 9 | 54.52 | 52.64 | 11 | 60.14 | 53.27 |
| 4 | M | 20 | 1 | 42.7 | 60.33 | 2 | 43.65 | 61.65 | 14 | 63.94 | 52.64 | 13 | 64.71 | 53.27 |
| 5 | F | 20 | 7 | 57.81 | 60.33 | 7 | 56.5 | 61.65 | 8 | 52.64 | 52.64 | 7 | 50.98 | 53.27 |
| 6 | M | 21 | 10 | 65.37 | 60.33 | 11 | 66.79 | 61.65 | 12 | 60.17 | 52.64 | 14 | 67 | 53.27 |
| 7 | M | 21 | 0 | 40.18 | 60.33 | 1 | 41.08 | 61.65 | 8 | 52.64 | 52.64 | 7 | 50.98 | 53.27 |
| 8 | M | 23 | 0 | 40.18 | 60.33 | 0 | 38.51 | 61.65 | 0 | 37.57 | 52.64 | 0 | 34.97 | 53.27 |
| 9 | F | 23 | 0 | 40.18 | 60.33 | 0 | 38.51 | 61.65 | 0 | 37.57 | 52.64 | 0 | 34.97 | 53.27 |
| 10 | M | 24 | 9 | 62.85 | 60.33 | 8 | 59.07 | 61.65 | 12 | 60.17 | 52.64 | 11 | 60.14 | 53.27 |
| 11 | M | 24 | 4 | 50.25 | 60.33 | 2 | 43.65 | 61.65 | 2 | 41.34 | 52.64 | 0 | 34.97 | 53.27 |
| 12 | M | 25 | 5 | 52.77 | 60.33 | 6 | 53.93 | 61.65 | 7 | 50.75 | 52.64 | 14 | 67 | 53.27 |
| 13 | M | 25 | 9 | 62.85 | 60.33 | 5 | 51.36 | 61.65 | 12 | 60.17 | 52.64 | 7 | 50.98 | 53.27 |
| 14 | M | 25 | 3 | 47.73 | 60.33 | 0 | 38.51 | 61.65 | 0 | 37.57 | 52.64 | 2 | 39.54 | 53.27 |
| 15 | M | 25 | 8 | 60.33 | 60.33 | 7 | 56.5 | 61.65 | 13 | 62.05 | 52.64 | 8 | 53.27 | 53.27 |
| 16 | M | 26 | 7 | 57.81 | 60.33 | 6 | 53.93 | 61.65 | 11 | 58.29 | 52.64 | 15 | 69.29 | 53.27 |
| 17 | M | 27 | 0 | 40.18 | 60.33 | 2 | 43.65 | 61.65 | 2 | 41.34 | 52.64 | 3 | 41.83 | 53.27 |
| 18 | M | 31 | 0 | 40.18 | 60.33 | 8 | 59.07 | 61.65 | 16 | 67.7 | 52.64 | 10 | 57.85 | 53.27 |
| 19 | F | 33 | 0 | 40.18 | 60.33 | 1 | 41.08 | 61.65 | 1 | 39.45 | 52.64 | 1 | 37.25 | 53.27 |
| 20 | M | 33 | 4 | 50.25 | 60.33 | 2 | 43.65 | 61.65 | 12 | 60.17 | 52.64 | 7 | 50.98 | 53.27 |
| 21 | M | 33 | 2 | 45.21 | 60.33 | 6 | 53.93 | 61.65 | 5 | 46.99 | 52.64 | 6 | 48.7 | 53.27 |
| 22 | M | 33 | 0 | 40.18 | 60.33 | 3 | 46.22 | 61.65 | 6 | 48.87 | 52.64 | 11 | 60.14 | 53.27 |
| 23 | F | 38 | 0 | 40.18 | 60.33 | 3 | 46.22 | 61.65 | 5 | 46.99 | 52.64 | 8 | 53.27 | 53.27 |
| 24 | F | 42 | 5 | 52.77 | 60.33 | 0 | 38.51 | 61.65 | 9 | 54.52 | 52.64 | 9 | 55.56 | 53.27 |
| 25 | F | 44 | 0 | 40.18 | 60.33 | 0 | 38.51 | 61.65 | 0 | 37.57 | 52.64 | 0 | 34.97 | 53.27 |
| 26 | M | 46 | 0 | 40.18 | 60.33 | 0 | 38.51 | 61.65 | 5 | 46.99 | 52.64 | 3 | 41.83 | 53.27 |
| 27 | F | 46 | 4 | 50.25 | 60.33 | 3 | 46.22 | 61.65 | 15 | 65.82 | 52.64 | 4 | 44.12 | 53.27 |
| 28 | F | 46 | 2 | 45.21 | 60.33 | 6 | 53.93 | 61.65 | 2 | 41.34 | 52.64 | 6 | 48.7 | 53.27 |
| 29 | F | 50 | 3 | 47.73 | 60.33 | 0 | 38.51 | 61.65 | 3 | 43.22 | 52.64 | 0 | 34.97 | 53.27 |
| 30 | M | 53 | 4 | 50.25 | 60.33 | 9 | 61.65 | 61.65 | 11 | 58.29 | 52.64 | 15 | 69.29 | 53.27 |
| Mean | 3.4 | 48.74 | 60.33 | 4.26 | 49.47 | 61.65 | 7.3 | 51.31 | 52.64 | 6.9 | 50.75 | 53.27 | ||
| Median | 3 | 47.73 | 60.33 | 3 | 46.22 | 7.5 | 51.69 | 7 | 50.98 | 53.27 | ||||
| Min | 0 | 40.18 | 0 | 38.51 | 0 | 37.57 | 0 | 34.97 | ||||||
| Max | 10 | 65.37 | 17 | 82.21 | 16 | 67.7 | 15 | 69.29 | ||||||
| Notes: Initials = The first letters of the name and surname of the participants; psychological scales - threshold; Low self-esteem - 60.33; Personal alienation – 61.65; Interpersonal insecurity – 52.64; Interpersonal alienation – 53.27; M = mean, m = median, min = minimum, max = maximum, th = threshold, red numbers = threshold limit exceeded, green numbers = threshold limit reached. | ||||||||||||||
It is observed that male athletes are less psychologically balanced than female athletes because only 3 female athletes exceeded at least one of the thresholds for the investigated psychological scales, while 10 male athletes exceeded at least one of the thresholds of a scale.
In Table 6, on the scale of interoceptive deficits, 7 athletes of which 32 juniors and 5 seniors obtained a rated score higher than the threshold value, while three other athletes (2 juniors and one senior) reached the threshold without exceeding it. On the emotional imbalance scale, 6 athletes (2 juniors and 4 seniors) exceeded the critical threshold and one obtained the same threshold value, being at the limit of specific symptoms. On the perfectionism scale, 10 athletes (3 juniors, 5 seniors, 2 athletes in the masters’ category) exceeded the threshold value, of which 4 athletes (one junior, one senior, and 2 athletes from the masters’ category, and one senior achieved the same threshold value, being at the limit of specific symptomatology.
| Table 6: The raw score/rated results and threshold for EDI -III – 9 psychological scales (DI, DE, P, A, and FM scales). | ||||||||||||||||
| No. crt. | Age | DI-rated | DI-threshold | DE-raw | DE-rated | DE-threshold | P-raw | P-rated | P-threshold | A-raw | A-rated | A-threshold | FM-raw | FM-crated | FM-raw | |
| M | 18 | 14 | 67.34 | 52.97 | 4 | 47.89 | 58.88 | 11 | 52.3 | 54.36 | 5 | 47.03 | 49.32 | 9 | 44.4 | 51.03 |
| M | 19 | 0 | 37.76 | 52.97 | 1 | 41.3 | 58.88 | 10 | 50.25 | 54.36 | 4 | 44.75 | 49.32 | 1 | 31.16 | 51.03 |
| M | 19 | 17 | 70.08 | 52.97 | 19 | 80.86 | 58.88 | 14 | 58.48 | 54.36 | 23 | 88.13 | 49.32 | 16 | 55.99 | 51.03 |
| M | 20 | 8 | 52.97 | 52.97 | 16 | 74.26 | 58.88 | 15 | 60.53 | 54.36 | 9 | 56.16 | 49.32 | 21 | 64.27 | 51.03 |
| F | 20 | 7 | 51.06 | 52.97 | 1 | 41.3 | 58.88 | 13 | 56.42 | 54.36 | 14 | 67.58 | 49.32 | 11 | 47.72 | 51.03 |
| M | 21 | 8 | 52.97 | 52.97 | 9 | 58.88 | 58.88 | 6 | 49.32 | 54.36 | 6 | 49.32 | 49.32 | 12 | 49.37 | 51.03 |
| M | 21 | 4 | 45.36 | 52.97 | 7 | 54.48 | 58.88 | 8 | 46.13 | 54.36 | 8 | 53.88 | 49.32 | 7 | 41.09 | 51.03 |
| M | 23 | 3 | 43.46 | 52.97 | 1 | 41.3 | 58.88 | 8 | 46.13 | 54.36 | 2 | 40.18 | 49.32 | 1 | 31.16 | 51.03 |
| F | 23 | 2 | 41.56 | 52.97 | 0 | 39.01 | 58.88 | 8 | 46.13 | 54.36 | 0 | 35.62 | 49.32 | 11 | 47.72 | 51.03 |
| M | 24 | 10 | 56.77 | 52.97 | 8 | 56.68 | 58.88 | 6 | 42.02 | 54.36 | 7 | 51.6 | 49.32 | 14 | 52.68 | 51.03 |
| M | 24 | 0 | 37.76 | 52.97 | 1 | 41.3 | 58.88 | 13 | 56.42 | 54.36 | 8 | 53.88 | 49.32 | 16 | 55.99 | 51.03 |
| M | 25 | 15 | 66.27 | 52.97 | 15 | 72.07 | 58.88 | 12 | 54.36 | 54.36 | 17 | 74.43 | 49.32 | 16 | 55.99 | 51.03 |
| M | 25 | 22 | 79.58 | 52.97 | 24 | 91.85 | 58.88 | 11 | 52.30 | 54.36 | 14 | 67.58 | 49.32 | 22 | 65.93 | 51.03 |
| M | 25 | 3 | 43.46 | 52.97 | 0 | 39.1 | 58.88 | 7 | 44.07 | 54.36 | 9 | 56.16 | 49.32 | 4 | 36.13 | 51.03 |
| M | 25 | 1 | 39.66 | 52.97 | 5 | 50.09 | 58.88 | 5 | 39.96 | 54.36 | 3 | 42.47 | 49.32 | 8 | 42.75 | 51.03 |
| M | 26 | 15 | 66.27 | 52.97 | 6 | 52.29 | 58.88 | 4 | 37.90 | 54.36 | 8 | 53.88 | 49.32 | 23 | 67.58 | 51.03 |
| M | 27 | 3 | 43.46 | 52.97 | 8 | 56.68 | 58.88 | 16 | 62.58 | 54.36 | 13 | 65.3 | 49.32 | 15 | 54.34 | 51.03 |
| M | 31 | 8 | 52.97 | 52.97 | 12 | 65.47 | 58.88 | 23 | 77.00 | 54.36 | 16 | 72.15 | 49.32 | 18 | 59.3 | 51.03 |
| F | 33 | 4 | 45.36 | 52.97 | 7 | 54.48 | 58.88 | 13 | 56.42 | 54.36 | 6 | 49.32 | 49.32 | 5 | 37.78 | 51.03 |
| M | 33 | 0 | 37.76 | 52.97 | 0 | 39.1 | 58.88 | 2 | 33.79 | 54.36 | 2 | 40.18 | 49.32 | 14 | 52.68 | 51.03 |
| M | 33 | 9 | 54.87 | 52.97 | 6 | 52.29 | 58.88 | 9 | 48.19 | 54.36 | 4 | 44.75 | 49.32 | 15 | 54.34 | 51.03 |
| M | 33 | 7 | 51.06 | 52.97 | 20 | 83.05 | 58.88 | 15 | 60.53 | 54.36 | 3 | 42.47 | 49.32 | 4 | 36.13 | 51.03 |
| F | 38 | 5 | 47.26 | 52.97 | 6 | 52.29 | 58.88 | 5 | 39.96 | 54.36 | 9 | 56.16 | 49.32 | 5 | 37.78 | 51.03 |
| F | 42 | 7 | 51.06 | 52.97 | 2 | 43.49 | 58.88 | 4 | 37.90 | 54.36 | 8 | 53.88 | 49.32 | 14 | 52.68 | 51.03 |
| F | 44 | 0 | 37.76 | 52.97 | 3 | 45.69 | 58.88 | 8 | 46.13 | 54.36 | 5 | 47.03 | 49.32 | 5 | 37.78 | 51.03 |
| M | 46 | 0 | 37.76 | 52.97 | 1 | 41.3 | 58.88 | 10 | 50.25 | 54.36 | 9 | 56.16 | 49.32 | 2 | 32.81 | 51.03 |
| F | 46 | 6 | 49.16 | 52.97 | 3 | 45.69 | 58.88 | 14 | 58.48 | 54.36 | 14 | 67.58 | 49.32 | 12 | 49.37 | 51.03 |
| F | 46 | 3 | 43.46 | 52.97 | 6 | 52.29 | 58.88 | 9 | 48.19 | 54.36 | 12 | 61.01 | 49.32 | 10 | 46.06 | 51.03 |
| F | 50 | 2 | 41.56 | 52.97 | 0 | 39.1 | 58.88 | 13 | 56.42 | 54.36 | 11 | 60.73 | 49.32 | 6 | 39.44 | 51.03 |
| M | 53 | 4 | 45.36 | 52.97 | 3 | 45.69 | 58.88 | 10 | 50.25 | 54.36 | 14 | 67.58 | 49.32 | 20 | 62.62 | 51.03 |
| 30 | M | 6.23 | 49.6 | 52.97 | 6.46 | 53.30 | 58.88 | 10.06 | 50.62 | 54.36 | 8.76 | 55.63 | 49.32 | 1123 | 48.10 | 51.03 |
| m | 4.5 | 46.31 | 52.97 | 5.5 | 51.19 | 58.88 | 10 | 50.25 | 54.36 | 8 | 53.88 | 49.32 | 115 | 48.54 | 51.03 | |
| min | 0 | 37.76 | 52.97 | 0 | 39.01 | 58.88 | 2 | 33.79 | 54.36 | 0 | 35.62 | 49.32 | 1 | 31.16 | 51.03 | |
| max | 22 | 79.58 | 52.97 | 24 | 91.85 | 58.88 | 23 | 77 | 54.36 | 23 | 88.13 | 49.32 | 23 | 67.58 | 51.03 | |
| Note: Initials = The first letters of the name and surname of the participants; psychological scales – threshold; DI = Interoceptive deficits – 52.97; DE = Emotional imbalance – 58.88; P=Perfectionism – 54.36; A= Asceticism – 49.32; FM = Fear of maturity – 51.03; M = mean, m = median, min = minimum, max = maximum, red numbers = threshold limit exceeded, green numbers = threshold limit reached. | ||||||||||||||||
On the asceticism scale, 19 athletes (4 juniors, 8 seniors, and 8 masters) obtained values above the threshold, of which 6 athletes (one junior and 5 masters), while 2 athletes (junior and one senior) reached the threshold value. On the fear of maturity scale, 13 athletes exceeded the critical threshold, of which 2 juniors, 9 seniors, and 2 athletes both female and male, from the masters’ category, not being athletes who reached their limit.
According to Table 7, female athletes obtained lower average values than male athletes on all investigated psychological scales, which indicates that they have higher self-esteem than male athletes, personal alienation, interpersonal insecurity, and lower interpersonal alignment than male athletes. The mean of the rated score for females did not exceed the critical threshold, while for males the threshold was exceeded on the interpersonal insecurity and interpersonal alienation scales. The average of the rated scores calculated for all athletes did not exceed the critical threshold, so the athletes who practice bodybuilding and fitness are well-balanced from a psychological point of view (Figures 5 and 6).
| Table 7: Centralization of threshold results, raw/rated score, and threshold for EDI-III-9 psychological scales (SSS, AP, NI, and AI scales). | ||||||||||||||
| EDI -III – 9 psychological scales, psychological scales | ||||||||||||||
| No. crt. | Means | Age | SSS-raw | SSS-rated | SSS-th | AP-raw | AP-rated | AP-th | NI-raw | NI-rated | NI-th | AI-raw | AI-crated | AI-th |
| 1 | Mean | F | 2,33 | 46,05 | 60,33 | 2,22 | 44,22 | 61,65 | 4,77 | 46,56 | 52,64 | 3,88 | 43,86 | 53,27 |
| 2 | Mean | M | 3,85 | 49,89 | 60,33 | 5,14 | 51,72 | 61,65 | 8,38 | 53.35 | 52,64 | 8,19 | 53.78 | 53,27 |
| 3 | Mean | F+M | 3,4 | 48,74 | 60,33 | 4,26 | 49,47 | 61,65 | 7,3 | 51,31 | 52,64 | 6,9 | 50,75 | 53,27 |
| Notes: Average female (F), male (M), F+M; psychological scales - threshold; Low self-esteem - 60.33; Personal alienation – 61.65; Interpersonal insecurity – 52.64; Interpersonal alienation – 53.27; th = threshold; red numbers = threshold limit exceeded. | ||||||||||||||
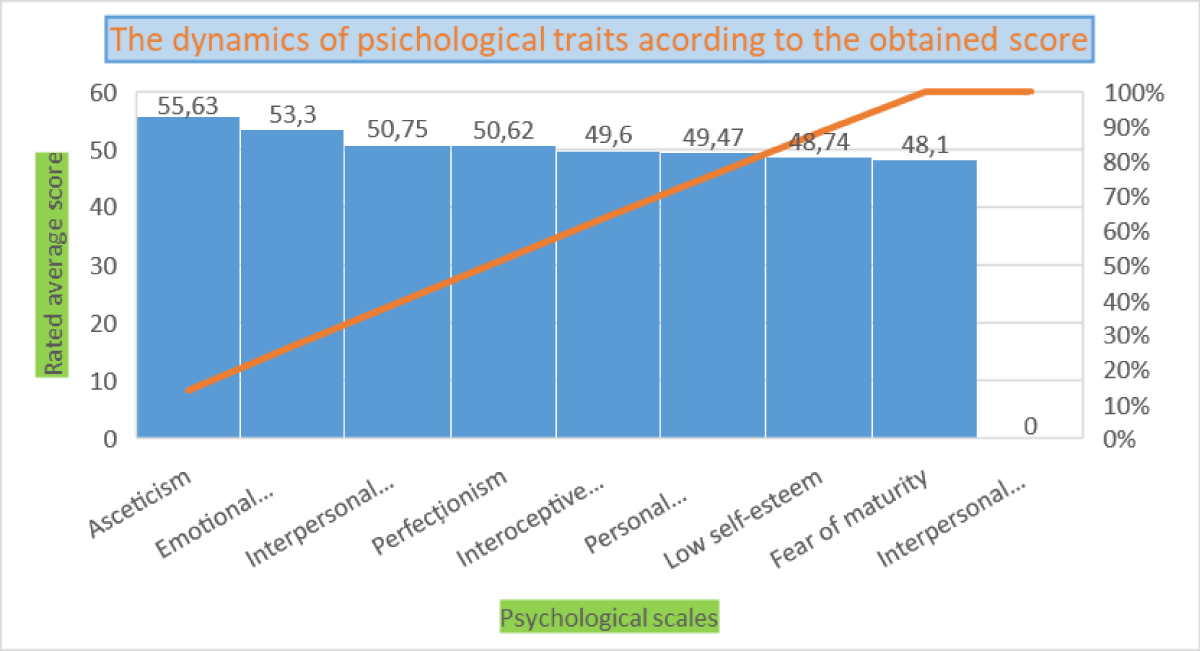
Figure 5: Graphical representation of the averages of the rated scores obtained on the psychological scales.
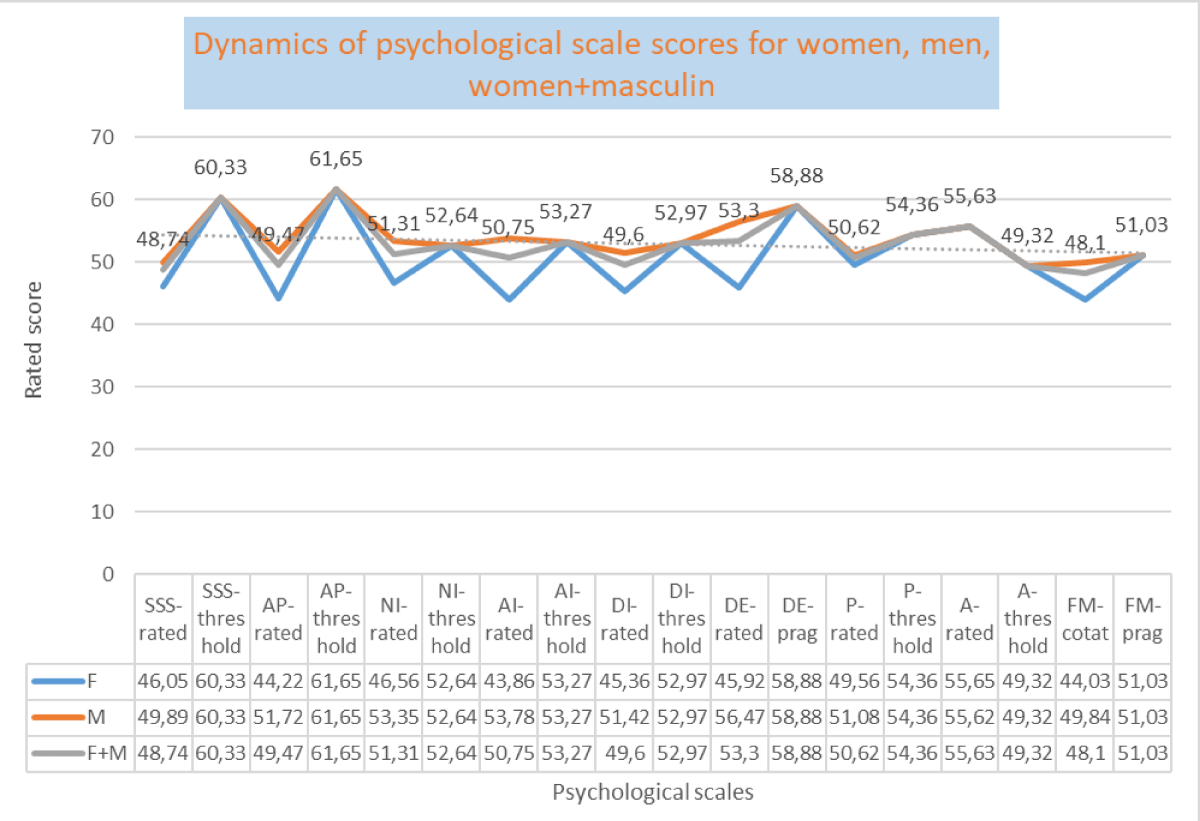
Figure 6: Graphical representation of the averages of the rated scores obtained on the psychological scales differentiated by female/male and undifferentiated sexes.
According to Table 8, the female athletes obtained a lower average rated value than the male athletes on the interoceptive deficit scales, with a difference of 5 points, emotional imbalance with a difference of 10 points, and on the perfectionism scale but with a small difference of almost two points, the female and male averages being close in value. On the asceticism scale, the female and male averages were almost equal, the critical threshold being exceeded in both cases, while on the other scales, the average score did not exceed the critical threshold. Female athletes have a lower fear of maturity than male athletes, with a difference of 5 points between the two averages (Figures 7 and 8).
| Table 8: Centralization of raw score/rated results and threshold for EDI -III – 9 psychological scales (DI, DE, P, A, and FM scales). | |||||||||||||||
| AverageF/M | DI-raw | DI-rated | DI-threshold | DE-raw | DE-rated | DE-threshold | P-raw | P-rated | P-threshold | A-raw | A-rated | A-threshold | FM-raw | FM-rated | FM-threshold |
| 9F | 4 | 45,36 | 52,97 | 3,11 | 45,92 | 58,88 | 9,66 | 49,56 | 54,36 | 8,77 | 55.65 | 49,32 | 8,77 | 44,03 | 51,03 |
| 21M | 7,19 | 51,42 | 52,97 | 7,9 | 56,47 | 58,88 | 10,23 | 51,08 | 54,36 | 8,76 | 55.62 | 49,32 | 12,28 | 49,84 | 51,03 |
| F+M | 6,23 | 49,6 | 52,97 | 6,46 | 53,30 | 58,88 | 10,06 | 50,62 | 54,36 | 8,76 | 55.63 | 49,32 | 11,23 | 48,10 | 51,03 |
| Notes: Average female (F), male (M), F+M; psychological scales: DI = Interoceptive deficits – 52.97; DE = Emotional imbalance – 58.88; P = Perfectionism – 54.36; A = Asceticism – 49.32; FM = Fear of maturity – 51.03, M = mean, th = threshold; red numbers = threshold limit exceeded. | |||||||||||||||

Figure 7: Example NPG threshold exceeded.
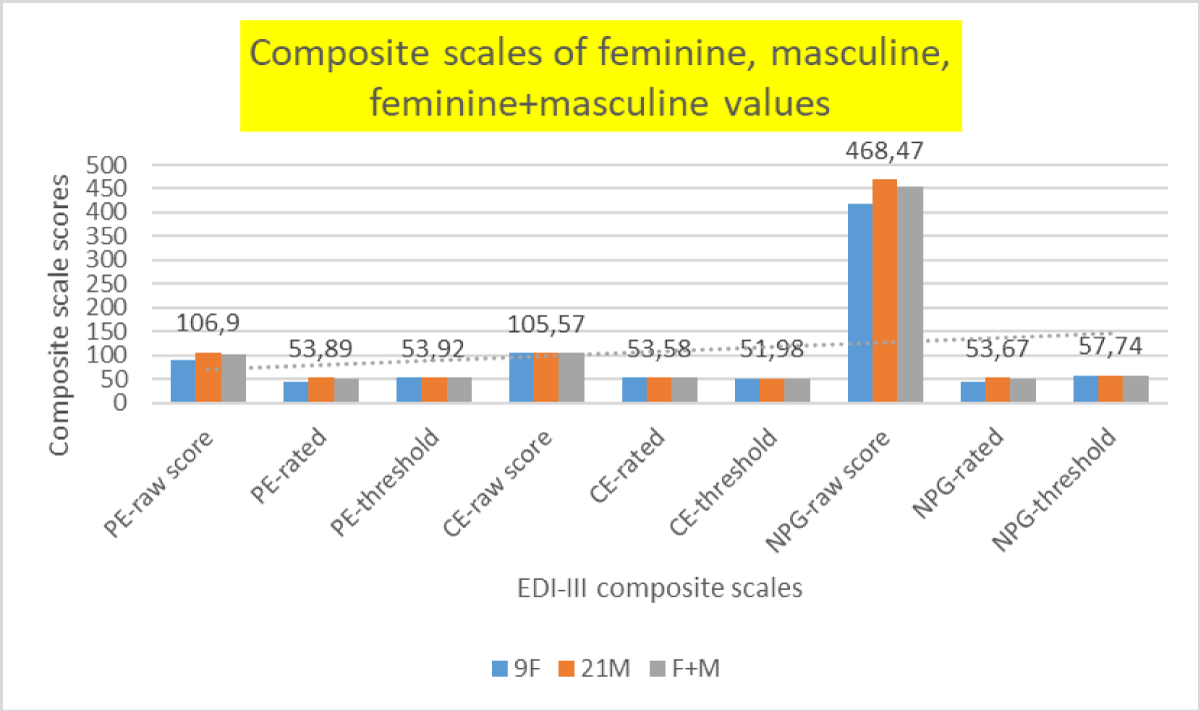
Figure 8: Graphical representation of the averages of the rated scores obtained on the composite scales.
The rated scores/percentages of specific scales and psychological scales from the inventory of eating behavior disorders - EDI -III for 30 athletes are presented in Table 14 and the results are represented in Figure 9.
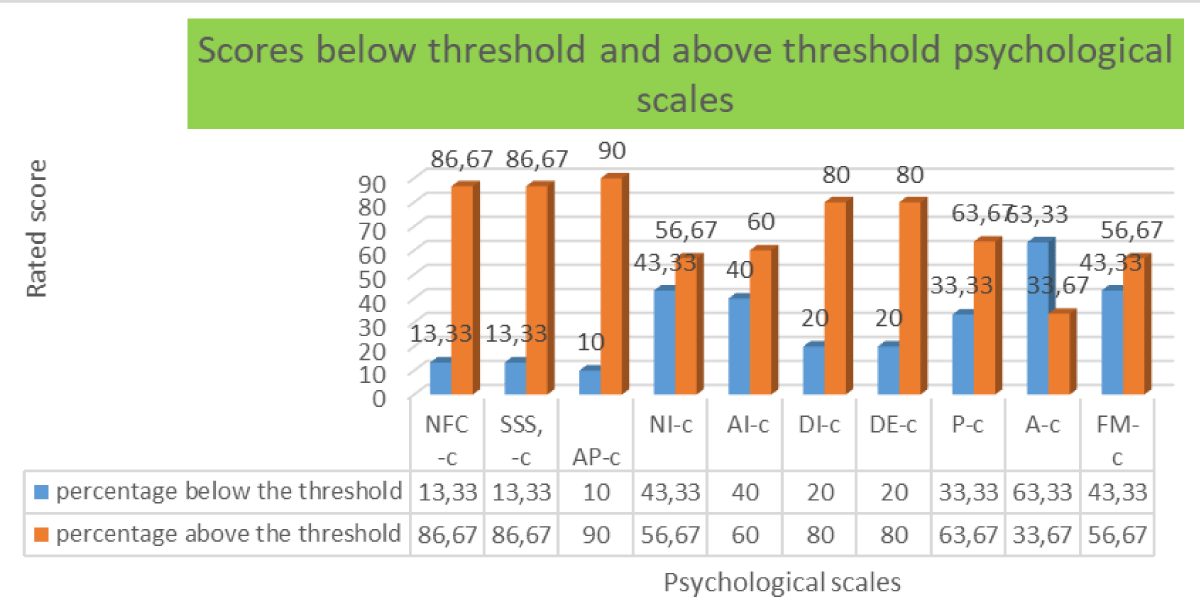
Figure 9: Graphical representation of average rated scores obtained on psychological scales.
c) EDI -III questionnaire - composite scales (COGNITROM, 2021, updated Copyright © 2023)
Composition scales – threshold
Risk of eating disorder - 61.29; Ineffectiveness - 60.72; Interpersonal problems - 49,41; Emotional problems - 53.92; Excessive control - 51.98; General psychological maladjustment - 57.74
The average has values above 48 for all 6 components, which reflects that the evaluated athletes obtained the average value of the rated score in general below the specified threshold for each evaluated component, as follows:
Scale: Risk of eating disorder (RCTA)
Interpretation: There are no significant problems with eating and body weight concerns - characterized by fear of gaining weight, a desire to be thinner, compulsive eating tendencies, and body dissatisfaction. A very low score may also reflect denial of the current clinical situation or distortions of responses.
Scale: Ineffectiveness (Inef)
Interpretation: Deep feelings of emotional emptiness and loneliness are not present; general self-assessment is positive.
Scale: Interpersonal problems (PI)
Interpretation: No significant or persistent interpersonal problems are found, Secure and reliable interpersonal attachments are present, which are satisfactory and generally of good quality. The person can feel support, understanding, and love in relationships.
Scale: Emotional problems (PE)
Interpretation: There are usually no significant or persistent problems in identifying, understanding, or responding correctly to emotional states, nor in terms of impulsivity, instability, liability, and dispositional intolerance. The person does not tend to respond to emotions through fear, confusion, or mistrust.
Scale: Exaggerated control (CE)
Interpretation: The person does not feel the need to reach certain high standards of performance and also does not experience virtue through self-denial, self-sacrifice, and suffering.
Scale: General psychological maladjustment (NPG)
Interpretation: The person does not usually experience or report an increased level of distress (negative emotional states) on the level of global psychological functioning, however, the score may reflect a general tendency to minimize psychological distress, rather than the absence of distress.
Interpretation: The presence of a significant level of distress (negative emotional states) is noted, including low self-esteem, personal alienation, interpersonal insecurity, interpersonal alienation, interoceptive deficits, emotional imbalance, perfectionism, asceticism, and fear of maturity. This score indicates the existence of significant dysfunctions, both in the personal and interpersonal psychological fields.
In Table 9, eating disorder risk was identified in 4 athletes, including 3 juniors (two juniors and one junior) and one senior who scored higher than the critical threshold of the scale. On the ineffectiveness scale, the critical threshold was exceeded by 4 athletes, respectively 3 juniors and one senior. Most of the exceeded thresholds resulted from the centralization of the results on the interpersonal problems scale, where 17 athletes (6 juniors, 8 seniors, 3 masters) obtained scores above the threshold, of which only two athletes (a junior and another from masters’ category), and one another athlete, also from the masters’ category, reached the limit. On this scale, the critical threshold was also exceeded for the average value of the rated scores obtained by the 30 athletes.
| Table 9: The raw score, rated score, and threshold for EDI -III – 6 composite scales (RCTA, Inef, and PI scales). | |||||||||||
| Sex | Initials | Age | RCTA-raw | RCTA-rated | RCTA-th | Inef.-raw | Inef-rated | Inef-th | PI-raw | PI-rated | PI-th |
| M | B | 18 | 180 | 62.08 | 61.29 | 133 | 67.7 | 60.72 | 136 | 70.42 | 49.41 |
| M | GA | 19 | 123 | 39.4 | 61.29 | 78 | 38.72 | 60.72 | 77 | 36.92 | 49.41 |
| M | RR | 19 | 190 | 66.06 | 61.29 | 137 | 69.85 | 60.72 | 114 | 57.93 | 49.41 |
| M | BV | 20 | 133 | 43.38 | 61.29 | 85 | 41.94 | 60.72 | 127 | 65.31 | 49.41 |
| F | MM | 20 | 195 | 68.05 | 61.29 | 113 | 56.97 | 60.72 | 102 | 51.11 | 49.41 |
| M | CA | 21 | 174 | 59.69 | 61.29 | 131 | 66.63 | 60.72 | 127 | 65.31 | 49.41 |
| M | TG | 21 | 144 | 47.76 | 61.29 | 81 | 39.79 | 60.72 | 102 | 51.11 | 49.41 |
| M | AC | 23 | 138 | 45.37 | 61.29 | 78 | 38.72 | 60.72 | 71 | 34.75 | 49.41 |
| F | NG | 23 | 142 | 46.96 | 61.29 | 78 | 38.72 | 60.72 | 71 | 34.65 | 49.41 |
| M | AA | 24 | 165 | 56.11 | 61.29 | 121 | 61.26 | 60.72 | 120 | 61.33 | 49.41 |
| M | OC | 24 | 148 | 49.35 | 61.29 | 93 | 46.23 | 60.72 | 75 | 35.78 | 49.41 |
| M | AR | 25 | 163 | 55.32 | 61.29 | 105 | 52.67 | 60.72 | 117 | 59.63 | 49.41 |
| M | CC | 25 | 168 | 57.31 | 61.29 | 113 | 56.97 | 60.72 | 110 | 55.66 | 49.41 |
| M | MT | 25 | 143 | 47.36 | 61.29 | 85 | 41.94 | 60.72 | 76 | 36.35 | 49.41 |
| M | SC | 25 | 135 | 44.17 | 61.29 | 116 | 58.58 | 60.72 | 115 | 58.5 | 49.41 |
| M | NN | 26 | 169 | 57.7 | 61.29 | 110 | 55.36 | 60.72 | 127 | 65.31 | 49.41 |
| M | FR | 27 | 126 | 40.59 | 61.29 | 83 | 40.86 | 60.72 | 82 | 39.76 | 49.41 |
| M | CV | 31 | 195 | 68.05 | 61.29 | 99 | 49.45 | 60.72 | 124 | 63.61 | 49.41 |
| F | LS | 33 | 139 | 45.77 | 61.29 | 81 | 39.79 | 60.72 | 76 | 36.35 | 49.41 |
| M | PS | 33 | 135 | 44.17 | 61.29 | 93 | 46.23 | 60.72 | 110 | 55.66 | 49.41 |
| M | PR | 33 | 144 | 47.76 | 61.29 | 98 | 48.92 | 60.72 | 94 | 46.57 | 49.41 |
| M | SC | 33 | 141 | 46.56 | 61.29 | 86 | 42.47 | 60.72 | 108 | 54.52 | 49.41 |
| F | GAG | 38 | 139 | 45.77 | 61.29 | 86 | 42.47 | 60.72 | 99 | 49.41 | 49.41 |
| F | KP | 42 | 157 | 52.93 | 61.29 | 90 | 44.62 | 60.72 | 109 | 55.09 | 49.41 |
| F | ME | 44 | 125 | 40.19 | 61.29 | 78 | 38.72 | 60.72 | 71 | 34.64 | 49.41 |
| M | PC | 46 | 132 | 42.98 | 61.29 | 78 | 38.72 | 60.72 | 87 | 42.6 | 49.41 |
| F | RA | 46 | 174 | 59.69 | 61.29 | 96 | 47.84 | 60.72 | 109 | 55.09 | 49.41 |
| F | ZAM | 46 | 154 | 51.73 | 61.29 | 98 | 48.92 | 60.72 | 89 | 43.73 | 49.41 |
| F | ND | 50 | 133 | 43.38 | 61.29 | 85 | 41.94 | 60.72 | 77 | 36.92 | 49.41 |
| M | BC | 53 | 139 | 45.77 | 61.29 | 111 | 55.89 | 60.72 | 127 | 65.31 | 49.41 |
| 30 | Mean | 151.43 | 50.71 | 61.29 | 97.3 | 48.62 | 60.72 | 100.96 | 50.64 | 49.41 | |
| Median | 143.5 | 47.56 | 61.29 | 93 | 46.23 | 60.72 | 105 | 52.81 | 49.41 | ||
| Min | 123 | 39.4 | 61.29 | 78 | 38.72 | 60.72 | 71 | 34.65 | 49.41 | ||
| Max | 195 | 68.05 | 61.29 | 137 | 69.85 | 60.72 | 136 | 70.42 | 49.41 | ||
| Notes: Composite-threshold scales: RCTA = Risk of eating disorder - 61.29; Inef = Inefficiency – 60.72; PI = Interpersonal problems- 49.41, th = threshold; red numbers = threshold limit exceeded; red numbers = threshold limit exceeded, green numbers = threshold limit reached. | |||||||||||
According to Table 10, on the scale of emotional problems, 10 athletes exceeded the critical threshold, of which 4 juniors and 6 seniors, the average rated score of the 30 athletes did not exceed the critical threshold. On the exaggerated control scale, 14 athletes (3 juniors, 6 seniors, and 5 masters) obtained values above the critical threshold, of which 5 athletes (one junior, one senior, and 3 masters), the large number of athletes who exceeded the critical threshold also led when exceeding the average score rated for 30 athletes on this scale.
| Table 10: The raw score, rated score, and threshold results for EDI -III – 6 composite scales (PE, CE, and NPG scales). | |||||||||||
| Sex | Initials | Age | PE-raw | PE-rated | PE-th | CE-raw | CE-rated | CE-th | NPG-raw | NPG-rated | NPG-th |
| M | NB | 18 | 111 | 56.15 | 53.92 | 99 | 49.5 | 51.98 | 523 | 63.09 | 57.74 |
| M | GA | 19 | 78 | 37.76 | 53.92 | 94 | 46.39 | 51.98 | 358 | 34.59 | 57.74 |
| M | RR | 19 | 150 | 77.89 | 53.92 | 146 | 78.73 | 51.98 | 602 | 76.74 | 57.74 |
| M | BV | 20 | 126 | 64.52 | 53.92 | 116 | 60.07 | 51.98 | 518 | 62.23 | 57.74 |
| F | MM | 20 | 92 | 45.56 | 53.92 | 123 | 64.42 | 51.98 | 477 | 55.15 | 57.74 |
| M | CA | 21 | 110 | 55.6 | 53.92 | 91 | 44.52 | 51.98 | 508 | 60.5 | 57.74 |
| M | TG | 21 | 99 | 49.46 | 53.92 | 99 | 49.5 | 51.98 | 422 | 45.64 | 57.74 |
| M | AC | 23 | 84 | 41.1 | 53.92 | 86 | 41.41 | 51.98 | 350 | 33.2 | 57.74 |
| F | NG | 23 | 80 | 38.87 | 53.92 | 81 | 38.3 | 51.98 | 357 | 34.41 | 57.74 |
| M | AA | 24 | 112 | 56.71 | 53.92 | 93 | 45.76 | 51.98 | 498 | 58.78 | 57.74 |
| M | OC | 24 | 78 | 37.76 | 53.92 | 109 | 55.72 | 51.98 | 410 | 43.57 | 57.74 |
| M | AR | 25 | 138 | 71.2 | 53.92 | 128 | 67.53 | 51.98 | 543 | 66.55 | 57.74 |
| M | CC | 25 | 170 | 89.04 | 53.92 | 119 | 61.93 | 51.98 | 577 | 72.42 | 57.74 |
| M | MT | 25 | 82 | 39.99 | 53.92 | 100 | 50.12 | 51.98 | 379 | 38.22 | 57.74 |
| M | SC | 25 | 89 | 43.89 | 53.92 | 81 | 38.3 | 51.98 | 443 | 49.27 | 57.74 |
| M | NN | 26 | 118 | 60.06 | 53.92 | 90 | 43.9 | 51.98 | 512 | 61.19 | 57.74 |
| M | FR | 27 | 99 | 49.46 | 53.92 | 127 | 66.91 | 51.98 | 445 | 49.62 | 57.74 |
| M | CV | 31 | 117 | 59.5 | 53.92 | 149 | 80.59 | 51.98 | 548 | 67.41 | 57.74 |
| F | LS | 33 | 99 | 49.46 | 53.92 | 105 | 53.23 | 51.98 | 398 | 41.5 | 57.74 |
M |
PS | 33 | 76 | 37.2 | 53.92 | 73 | 33.33 | 51.98 | 404 | 42.53 | 57.74 |
M |
PR | 33 | 106 | 53.37 | 53.92 | 92 | 45.14 | 51.98 | 444 | 49.45 | 57.74 |
M |
SC | 33 | 134 | 68.97 | 53.92 | 102 | 51.36 | 51.98 | 466 | 53.25 | 57.74 |
F |
GAG | 38 | 99 | 49.46 | 53.92 | 95 | 47.01 | 51.98 | 416 | 44.61 | 57.74 |
F |
KP | 42 | 94 | 46.68 | 53.92 | 90 | 43.9 | 51.98 | 435 | 47.89 | 57.74 |
F |
ME | 44 | 82 | 39.99 | 53.92 | 93 | 45.76 | 51.98 | 361 | 35.11 | 57.74 |
M |
PC | 46 | 78 | 37.76 | 53.92 | 106 | 53.85 | 51.98 | 381 | 38.56 | 57.74 |
F |
RA | 46 | 94 | 46.68 | 53.92 | 125 | 65.67 | 51.98 | 473 | 54.46 | 57.74 |
F |
ZAM | 46 | 95 | 47.24 | 53.92 | 111 | 56.96 | 51.98 | 439 | 48.58 | 57.74 |
F |
ND | 50 | 80 | 38.87 | 53.92 | 116 | 60.07 | 51.98 | 397 | 41.33 | 57.74 |
M |
BC | 53 | 90 | 44.45 | 53.92 | 117 | 60.69 | 51.98 | 507 | 60.33 | 57.74 |
30 |
Mean | 102 | 51.15 | 53.92 | 105.2 | 53.35 | 51.98 | 453.03 | 51.06 | 57.74 | |
| Median | 97 | 48.35 | 53.92 | 101 | 50.74 | 51.98 | 443.5 | 49.36 | 57.74 | ||
| Min | 76 | 37.2 |
53.92 |
73 | 33.33 |
51.98 |
350 | 33.2 |
57.74 |
||
| Max | 170 | 89.04 |
53.92 |
149 | 80.59 |
51.98 |
602 | 76.74 |
57.74 |
||
Notes: Scales composition – threshold: PE = Emotional problems – 53.92; CE=Excessive control – 51.98; NPG = General psychological maladjustment – 57.74, th = threshold; red numbers = threshold limit exceeded, green numbers = threshold limit reached. |
|||||||||||
The premise of general psychological maladjustment can be further analyzed for a number of 10 athletes who exceeded the critical threshold, of which 4 juniors, 5 seniors, and 1 masters’ category, however the average result of the rated scores was below the critical threshold value, which means we can add the fact that for women there were no thresholds exceeded on this scale.
We can see in Table 11, that for women, no critical threshold of the RCTA, Inefficiency, and interpersonal problems scales was exceeded, while for men, the critical threshold was exceeded for the scale of interpersonal problems with 5 points, which is why the rated score of the 30 athletes exceeded this threshold.
| Table 11: Centralization of the raw score, rated score, and threshold for EDI -III –6 composite scales (RCTA, Inef, and PI scales). | ||||||||||
| Nr. crt. | Average F/M | RCTA-raw | RCTA-rated | RCTA-th | Inef.-raw | Inef-rated | Inef-th | PI-raw | PI-rated | PI-th |
| 1 | 9F | 150.88 | 50.49 | 61.29 | 89.44 | 44.44 | 60.72 | 89.22 | 44.11 | 49.41 |
| 2 | 21M | 151.66 | 50.8 | 61.29 | 100.66 | 50.42 | 60.72 | 106 | 53.44 | 49.41 |
| 3 | F+M | 151.43 | 50.71 | 61.29 | 97.3 | 48.62 | 60.72 | 100.96 | 50.64 | 49.41 |
| Notes: Average female (F), male (M), F+M; composite-threshold scales: RCTA = Risk of eating disorder - 61.29; Inef = Inefficiency – 60.72; PI = Interpersonal problems- 49.41, th = threshold; red numbers = threshold limit exceeded, green numbers = threshold limit reached. | ||||||||||
In Table 12, we can see that female athletes (rated score 44.75) have fewer emotional problems than male athletes (rated score 53.89) with approximately 9 points, a result similar to the results of the general psychological maladjustment scale, while on the exaggerated control scale both females (rated score 52, 81) as well as for males (rated score 53.58), the average rated scores exceeded the critical threshold (51.98), the difference between the scores being lower by one point for sportswomen compared to sportswomen for the values obtained regarding behaviors specific to exaggerated control (Figure 8).
| Table 12: Centralization of raw score results, rated score, and threshold for EDI -III – 6 composite scales (PE, CE, and NPG scales). | |||||||||||
| No. crt. | Average F/M | PE-raw | PE-rated | PE-th | CE-raw | CE-rated | CE-th | NPG-raw | NPG-rated | NPG-th | |
| 1 | 9F | 90.55 | 44.75 | 53.92 | 104.33 | 52.81 | 51.98 | 417 | 44.78 | 57.74 | |
| 2 | 21M | 106.9 | 53.89 | 53.92 | 105.57 | 53.58 | 51.98 | 468.47 | 53.67 | 57.74 | |
| 3 | F+M | 102 | 51.15 | 53.92 | 105.2 | 53.35 | 51.98 | 453.03 | 51.06 | 57.74 | |
| Notes: Average female (F), male (M), F+M. Composite scales – threshold: PE=Emotional problems – 53.92; CE = Excessive control – 51.98; NPG = General psychological maladjustment – 57.74, th = threshold; red numbers = threshold limit exceeded, green numbers = threshold limit reached. | |||||||||||
d) The EDI-III questionnaire - validity scales (COGNITROM, 2021, updated Copyright © 2023), which refers to the way to complete the questionnaire:
Scale: Inconsistency (I)
Interpretation: Consistency in answers (similar answers to questions with similar content);
Scale: Rarity (R)
Interpretation: No affirmative answers are given to questions probing severe symptoms;
Scale: Negative impression (IN)Interpretation: The intention of the evaluated person to present in an exaggerated manner the psychological states or traits of the person is not established.
According to Table 13, on the Inconsistency scale, 5 athletes, 3 of whom fall into the atypical category, respectively a junior, a senior, and a masters’ category, and 2 very atypical, respectively a junior and a senior. On the Rarity scale, a total of 7 athletes exceeded the critical threshold, of which 5 were atypical (2 juniors, 2 seniors, and 1 masters’ category) and 2 very atypical, both seniors, which signifies the presence of the relevant symptomatology of eating behavior disorders, in their case being necessary, the clarification of some aspects related to the understanding and the answer to the questions to which they answered positively and the repetition of the inventory at an interval of 6 months, and in the case of similar results, it is possible to intervene through psychological counseling or specialized psychiatric intervention. On the negative impression scale, 3 athletes obtained values above the threshold, respectively 1 junior and 2 seniors. 2 athletes, of which a junior and a senior exceeded all the validity thresholds of the Eating Disorders Inventory, results that call for further investigation and it is necessary to repeat the test and clarify some statements if their meaning was misinterpreted.
| Table 13: The resulting raw score, rated score, and threshold for EDI -III – 3 validity scales (I, R, and IN scales) | |||||||||||
| Sex | Initials | Age | I-raw | I-category | I-threshold | R-raw | R-category | R-threshold | IN-raw | IN-category | IN-threshold |
| M | NB | 18 18 18 | 15 | atypically | 15 | 0 | typical | 2 | 4 | typical | 14 |
| M | GA | 19 | 3 | typical | 15 | 0 | typical | 2 | 0 | typical | 14 |
| M | RR | 19 | 27 | atypically | 15 | 2 | atypically | 2 | 26 | atypically | 14 |
| M | BV | 20 | 4 | typical | 15 | 2 | atypically | 2 | 4 | Typical | 14 |
| F | MM | 20 | 9 | typical | 15 | 0 | typical | 2 | 5 | typical | 14 |
| M | CA | 21 | 8 | typical | 15 | 1 | typical | 2 | 2 | typical | 14 |
| M | TG | 21 | 9 | typical | 15 | 0 | typical | 2 | 0 | typical | 14 |
| M | AC | 23 | 7 | typical | 15 | 0 | typical | 2 | 1 | typical | 14 |
| F | NG | 23 | 1 | typical | 15 | 0 | typical | 2 | 2 | typical | 14 |
| M | AA | 24 | 11 | typical | 15 | 1 | typical | 2 | 1 | typical | 14 |
| M | OC | 24 | 8 | typical | 15 | 1 | typical | 2 | 7 | typical | 14 |
| M | AR | 25 | 14 | typical | 15 | 0 | typical | 2 | 7 | typical | 14 |
| M | CC | 25 | 11 | typical | 15 | 4 | atypically | 2 | 27 | atypically | 14 |
| M | MT | 25 | 7 | typical | 15 | 0 | typical | 2 | 2 | typical | 14 |
| M | SC | 25 | 16 | atypically | 15 | 0 | typical | 2 | 2 | typical | 14 |
| M | NN | 26 | 13 | typical | 15 | 2 | atypically | 2 | 12 | typical | 14 |
| M | FR | 27 | 3 | typical | 15 | 0 | typical | 2 | 9 | typical | 14 |
| M | CV | 31 | 20 | atypically | 15 | 4 | atypically | 2 | 24 | atypically | 14 |
| F | LS | 33 | 2 | typical | 15 | 0 | typical | 2 | 2 | typical | 14 |
| M | PS | 33 | 9 | typical | 15 | 1 | typical | 2 | 2 | typical | 14 |
| M | PR | 33 | 7 | typical | 15 | 1 | typical | 2 | 1 | typical | 14 |
| M | SC | 33 | 8 | typical | 15 | 2 | atypically | 2 | 8 | typical | 14 |
| F | GAG | 38 | 4 | typical | 15 | 0 | typical | 2 | 0 | typical | 14 |
| F | KP | 42 | 8 | typical | 15 | 0 | typical | 2 | 1 | typical | 14 |
| F | ME | 44 | 1 | typical | 15 | 0 | typical | 2 | 0 | typical | 14 |
| M | PC | 46 | 3 | typical | 15 | 0 | typical | 2 | 2 | typical | 14 |
| F | RA | 46 | 14 | typical | 15 | 0 | typical | 2 | 6 | typical | 14 |
| F | ZAM | 46 | 7 | typical | 15 | 0 | typical | 2 | 5 | typical | 14 |
| F | ND | 50 | 9 | typical | 15 | 0 | typical | 2 | 1 | typical | 14 |
| M | BC | 53 | 18 | atypically | 15 | 3 | atypically | 2 | 6 | typical | 14 |
| Notes: validity scales typical/atypical category – threshold: Inconsistency - I threshold 15, Rarity - R threshold 2; Negative impression – IN threshold 14. | |||||||||||
The percentages of composite scales and validity scales from the inventory of eating behavior disorders - EDI -III for 30 athletes are presented in Tables 14,15 and these results are represented in Figure 10.
| Table 14: Table of rated scores/percentages of specific scales and psychological scales from the inventory of eating behavior disorders - EDI -III for 30 athletes. | |||||||||||
| Psychological scales | |||||||||||
| No. crt. | Threshold | NFC-c | SSS-c | AP-c | NI-c | AI-c | DI-c | DE-c | P-c | A-c | FM-c |
| No. athletes | <th | 4 | 4 | 3 | 13 | 12 | 6 | 6 | 10 | 19 | 13 |
| >th | 26 | 26 | 27 | 17 | 18 | 24 | 24 | 20 | 11 | 17 | |
| % | <th | 13.33 | 13.33 | 10.00 | 43.33 | 40.00 | 20.00 | 20.00 | 33.33 | 63.33 | 43.33 |
| >th | 86.67 | 86.67 | 90.00 | 56.67 | 60.00 | 80.00 | 80.00 | 63.67 | 33.67 | 56.67 | |
| Notes: Psychological scales: Low self-esteem - 60.33; Personal alienation – 61.65; Interpersonal insecurity – 52.64; Interpersonal alienation – 53.27, Interoceptive deficits – 52.97; Emotional imbalance – 58.88; Perfectionism – 54.36; Asceticism – 49.32; Fear of maturity – 51.03, th = threshold. | |||||||||||
| Table 15: Table of percentages of composite scales and validity scales from the inventory of eating behavior disorders - EDI -III for 30 athletes. | ||||||||||
| No. crt. | Threshold | RCTA-rated | Inef-rated | PI-rated | PE-rated | CE-crated | NPG-crated | I-category | R-category | In-category |
| NS | >th | 4 | 4 | 17 | 10 | 14 | 10 | 5 (3a+2fa) | 7(5a+2fa) | 3 |
| <th | 26 | 26 | 13 | 20 | 16 | 20 | 25 | 23 | 27 | |
| % | >th | 13.33 | 13.33 | 56.67 | 33.33 | 46.67 | 33.33 | 6.67 | 23.33 | 10 |
| <th | 86.67 | 86.67 | 43.33 | 66.67 | 54.33 | 66.67 | 23.33 | 76.67 | 20 | |
| Notes: composite-threshold scales: Risk of eating disorder - 61.29; Inefficiency – 60.72; Interpersonal problems - 49.41, Emotional problems - 53.92; Excessive control – 51.98; General psychological maladjustment – 57.74, validity. scales=typical/atypical category – threshold: Inconsistency – I threshold 15; Rarity – R threshold 2; Negative impression – IN 14, NS = number of athletes, th = threshold. | ||||||||||
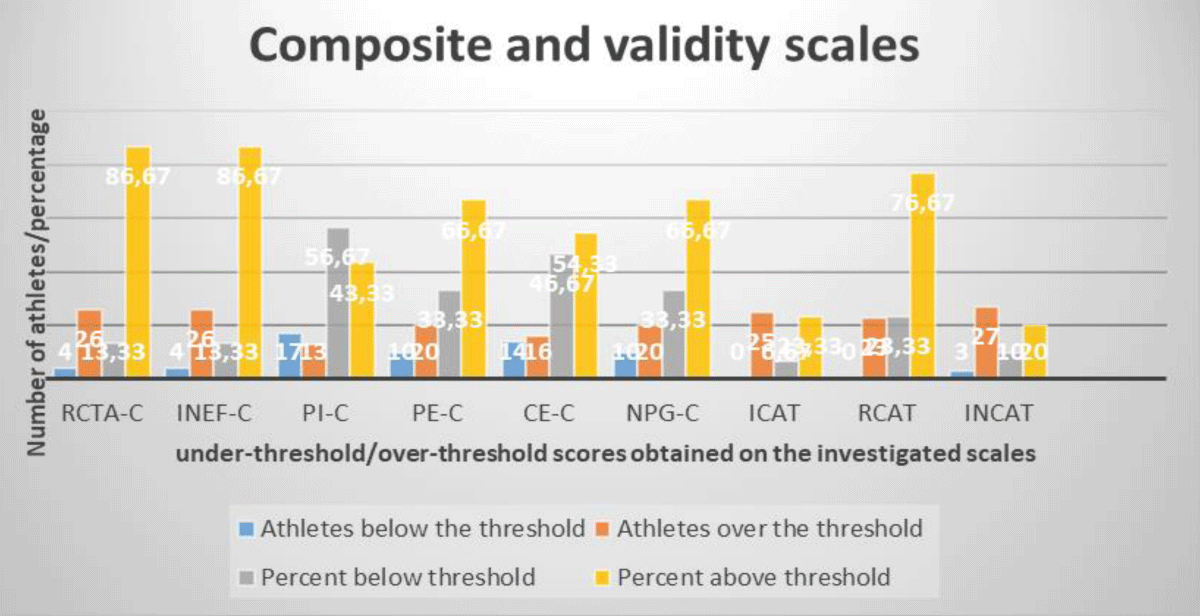
Figure 10: Graphical representation of the averages of the rated scores obtained on the composite and validity scales.
Most athletes have higher education, as seen in Table 16, out of the 30 athletes, 25 have higher education, of which 6 are bodybuilding and fitness instructors/personal trainers, one is an ABA Therapist, one is a university professor, 3 are engineers, and others have occupations with higher education or self-employed/freelance professionals. Of the 5 athletes who have secondary education, 2 are self-employed, one athlete is a civil servant, one is a student and one is unemployed.
| Table 16: List of sports subjects – ID generated by CAS++ application/occupation/studies/region. | ||||||
| Subject ID | Age | Sex | School Preparation | Status occupational | Region | |
| 8E2108B53CF68C2900EDB4EF | 18 | male | high school | student | - | Bucharest |
| D426DD91E5FB3E7BFAF99894 | 19 | male | high school | unemployed | - | Sibiu |
| 3DA6E072E515854E331CDBEA | 19 | male | higher education | student | - | Bucharest |
| 600A994C3DDF2EA3B3B4DCE1 | 20 | male | higher education | student | - | Bucharest |
| 229FBE6E99AFE16E112EFCC4 | 20 | female | higher education | student | - | Bucharest |
| 0D0B1A81DF05DFF397C7CAD3 | 21 | male | high school | on their own/self-employed | - | Sibiu |
| 5B07B277ADCBFE82319EC2FC | 22 | male | high school | on their own/self-employed | - | Sibiu |
| CE4DC3BA478798F76CA8EF67 | 23 | female | higher education | occupation with higher education | - | Bucharest |
| 2DB40A741D2C6130E33B7196 | 23 | female | higher education | occupation with higher education | ABA Therapist | Bucharest |
| 7B2E047B3002FB9F16E6BF1D | 24 | male | higher education | on their own/self-employed | Personal trainer | Bucharest |
| AFA7394124B80E06E1D9B835 | 24 | male | higher education | on their own/self-employed | - | Bucharest |
| C8BA602E027BA1DD5BE2AE98 | 25 | male | higher education | technician, foreman,office clerk | - | Bucharest |
| E27CA50AB56DCB07869CCDB1 | 25 | male | higher education | technician, foreman,office clerk | - | Bucharest |
| 93B9536EDFA60CAC76806227 | 25 | male | high school | on their own/self-employed | - | Bucharest |
| B92CFDB832C4D06729B2FFAB | 25 | male | higher education | occupation with higher education | engineer | Bucharest |
| 02754610CE30510AB8CF8819 | 25 | male | higher education | occupation with higher education | Personal trainer | Bucharest |
| 0E4091C7E289D66064954589 | 27 | male | higher education | on their own/self-employed | - | Bucharest |
| F18C876EDD59E3A20CF96A21 | 27 | male | higher education | on their own/self-employed | - | Bucharest |
| 78ADEFD37E0A4C424260C688 | 31 | male | higher education | on their own/self-employed | Personal trainer | Bucharest |
| 4D5ABC143EA2BC259C2BEEB6 | 33 | male | higher education | occupation with higher education | - | Bucharest |
| 61D979311C18CCD0F1C31EAA | 33 | male | higher education | on their own/self-employed | - | Bucharest |
| 8462448CB97313906E80C551 | 34 | male | higher education | occupation with higher education | technical support engineer | Bucharest |
| CE05D4F32147B02ABD563BC3 | 37 | female | higher education | occupation with higher education | insurance inspector | Bucharest |
| B682CB91B27E46515CDA30BA | 41 | female | high school | technician, foreman,office clerk | public servant | Sibiu |
| B50531A05B9544E42FA280D7 | 44 | female | higher education | occupation with higher education | Professor, kinetic Therapist | Maneciu-Prahova |
| C281940194D087919D293A3A | 46 | male | higher education | occupation with higher education | engineer | Maneciu-Prahova |
| 192BCF91BA57022E3B8F1DBA | 46 | female | higher education | occupation with higher education | Personal trainer | Bucharest |
| 837FF090B69164CE689D40B7 | 47 | female | higher education | occupation with higher education | - | Bucharest |
| 4ECAC6D3FA59708E6CBBEEEA | 49 | female | higher education | occupation with higher education | economist | Bucharest |
| D0646AA41359486E0FA7A1AE | 53 | male | higher education | occupation with higher education | teacher | Bucharest |
The region represents the place where they were tested, where they train, namely bodybuilding and fitness rooms in Bucharest, in Prahova county, as well as at the Bodybuilding and Fitness Championship in Sibiu, September 2021, Sports Hall.
Self-esteem is not the first reason men become competitive amateur bodybuilders, emulation was the largest category stated for starting bodybuilding (n = 118), followed by previous participation in sports (n = 107), self-esteem (n = 107). = 50), health (n = 36), and other (n = 28), concluded [7] by studying the reasons why men become competitive amateur bodybuilders.
The study exploring issues of identity construction in mature bodybuilders [15] seeks to contribute empirically, theoretically, and methodologically to the literature on aging bodies and identity construction by analyzing self-photographic data from a project exploring the embodied identities of mature bodybuilders, identified three important identities that participants constructed through the self-photograph task. These identities were; a healthy body-self, a performing body-self, and a relational body-self. In combination, these three identities provide insight into what mature bodybuilders themselves consider important in their lives and social worlds.
Bodybuilding was seen as a subcultural lifestyle of peripheral youth [16], in a qualitative study of a group of young Polish bodybuilders conducted in 2014 in a small town in North-Eastern Poland that still faces the consequences of the collapse of communism. The author found that bodybuilding activities provided instant gratification. Such activities allowed individuals to see the immediate effect of training. However, while these activities provided individuals with a way to develop a desirable sculpted body, they also led to distortions in their self-image and their daily lives, which in turn caused a postponement of engaging in typical mandated adult roles and instead a focus on the individual’s role and position within his or her peer group
The attitude of a winner, combativeness, and overcoming one’s limits through self-determination, combined with compliance with the training program, the diet, the controlled administration of nutritional supplements, and sufficient rest are extremely important aspects of the preparation of bodybuilders to participate in competitions. In this sense, the “Experiences of competitive male bodybuilders from a non-pathologizing perspective” [17] were analyzed using a meaning condensation procedure that resulted in five themes: being proud of the ability to discipline, seeing an attitude perfectionist as a necessary evil, experiencing recognition within the bodybuilding community, being stigmatized outside the bodybuilding community, and taking the stage to demonstrate a capacity for will and discipline. We suggest that bodybuilders can be stigmatized for violating social norms: through their distinctive appearance, through the way they deal with suspected drug use, and through challenging gender norms.
Other extremely important and interesting international studies that are too little initiated regarding the perspectives of self-determination theory in our country, such as [18], investigated the reasons for the practice and motivational regulations of men and women engaged in training through a descriptive cross-sectional study of 252 weight training participants (133 men and 119 women). The findings of this study highlight that men and women are self-determined to practice weight training and weight loss is positively associated with introjected regulation and muscle growth in women and men for the reason of “health and well-being”.
The affective states caused by the atmosphere in which the training takes place (musical background, easy communication, aesthetics of the participants, and the conditions in the hall), generate in the being of practitioners joy, enthusiasm, emulation, confidence, and desire for success, combativeness, stress reduction as well as a state of relaxation.
Another study similar to our authors’ initiative [19], tested the relationship between integrative motivation and the reasons for practicing physical exercises according to the frequency and type of practice, in a number of 358 subjects trained in gyms, by performing guided exercises and bodybuilding exercises, integrative motivation and reasons for practicing were measured. After descriptive and differential analysis, the data showed that people who participated in fitness programs were more concerned with image and social recognition.
A study topic similar to our research was initiated by researchers from Spain, [20] who analyzed the differences in personality traits of the participants, respectively 218 (competitive, non-competitive, and sedentary bodybuilders), confirming differences between the researched groups in regarding the investigated personality factors: reasoning, sensitivity, abstraction, on the other hand, the participants from the two active groups obtaining a higher score on the perfectionism factor.
The study on eating disorders of bodybuilding athletes after competitions [21], filling the existing gaps in the exploration of the condition on this subject, academically evolved that the culture group analyzed had 18.8% of participants at risk of developing eating disorders based on the applied questionnaire (EAT-26), a significant percentage compared to the total sample. The manifestation of eating disorders in athletes who practice bodybuilding and fitness, before, during, or even after competitions, is a theme still little explored in the scientific environment, highlighting the need for more detailed and in-depth studies on the subject in question.
Competitive bodybuilders use a combination of resistance training, cardiovascular exercise, calorie reduction, supplementation regimens, and peak strategies to lose fat mass and maintain fat-free mass. Although recommendations for contest preparation exist, applied research is limited, and data on bodybuilders’ contest preparation regimens are limited to case studies or small cohorts. Furthermore, the influence of different nutritional strategies on competitive performance is unknown. The average training time for a competitor was 22 +/- 9 weeks, the authors [22] concluded, with the nutrient intake of bodybuilders reflecting a high-protein, low-fat diet, total carbohydrate, protein, and fat intake decreased during the study for both males and females.
The authors [23] of a groundbreaking study attempted to find psychophysiological data to support one of the classifications of excessive bodybuilding as a pathological syndrome based on two different theories: bodybuilding as an addiction or as a Muscle Dysmorphic Disorder (MDD). No task-related differences were identified between groups with greater activation of the Dorsolateral Prefrontal Cortex (DLPFC) and Orbitofrontal Cortex (OFC) while viewing bodies and exercise equipment, but significantly greater activation was observed in bodybuilders in the Primary Somatosensory Cortex (PSC) and the left hemisphere Supplementary Motor Area (SMA) while viewing body images (under different conditions), meaning that these neurophysiological results could be interpreted as a first evidence for the MDD theory of bodybuilding excessive.
Bodybuilding is a sport that challenges the individual both physically and mentally. The fact that this sport requires significant investment, shaped by physical activity and diet, in one’s body can affect body perception over time. The authors [24] of a study tangent to our research investigated the relationship between sports motivation, muscle perception disorder, and orthorexia nervosa in male individuals involved in bodybuilding, the results led to the conclusion that people who engage in bodybuilding have greater intrinsic motivation than extrinsic motivation, and as muscle perception disorder increases, so will orthorexia neurosis (p < 0.05).
The extreme physical traits of successful female athletes suggest that this population may be particularly at risk for developing Eating Disorders (EDs), suggest the authors [25] of a study similar to ours to determine whether female athletes in the major bikini, fitness, figure and bodybuilding divisions were at risk of ED and to explore possible associated risk factors. Athletes who scored above the cutoff values for one or more of the EDI subscales or who engaged in at least one of the most concerning PWCM (binge eating, laxative use, and self-induced vomiting) were considered at risk for ED. Approximately half of the participants were identified with ED (46.6%), regardless of division, with 27.3% presenting with clinical ED and 19.3% with subclinical ED. Additionally, approximately half (48.9%) of participants had engaged in at least one of the most worrisome PWCMs in the past three months, with a smaller proportion (5.2%) engaging in all three PWCMs. Weak but significant correlations were found between some EDI subscales and reason for participating in sports, BMI, and body composition goals. The desire for thinness and body dissatisfaction were positively associated with PWCM use.
Competitive bodybuilders must adhere to an individualized training program for optimal results and athletic fitness, as well as a well-structured diet based on their metabolism and category, often aided by muscle-building or fat-burning drugs, culminating in a posing competition on stage.
Despite these rigorous requirements, competitive bodybuilding is popular, with thousands of competitions held annually around the world. In a circumspect analysis, in the study “Competitive Bodybuilding: Fitness, Pathology or Both?” [26], the authors believe that although many studies have addressed the psychological features of various sports and the athletes who compete in them, few have examined the psychological aspects of bodybuilding. Even fewer studies have specifically examined competitive bodybuilders as opposed to the much larger group of non-competing “recreational” bodybuilders. The limited available literature suggests that competitive bodybuilders may be at increased risk for four categories of psychopathology: muscle dysmorphia, eating disorders, abuse of appearance and performance-enhancing drugs, and exercise addiction. However, within each of these categories, one must carefully distinguish between planned and dedicated behaviors necessary for success in sport, as opposed to frankly pathological behaviors that impair social or professional function, cause subjective distress, or lead to negative consequences for health.
Studies on Muscle Dysmorphia (MD) have mostly focused on men. However, a new ideal body for women is emerging: a highly toned, athletic body with smooth, flat muscles. The focus on muscularity is a contributor to increased MD symptoms in women, in which it was [27] assessed the factor structure and psychometric properties of the Muscle Dysmorphic Disorder Inventory (MDDI) in two samples of physically active Italian women. Confirmatory factor analysis findings showed a three-factor structure with acceptable fit and invariance across groups. Omega coefficients revealed adequate internal consistency for all scales and for the MDDI total score. In addition, convergent and divergent validity as well as test-retest reliability were found to be good.
Bodybuilding athletes’ passion for a symmetrical, lean, strong, and muscular body leads them to perform grueling exercise programs and restrictive diets, sometimes leading to disordered eating behaviors. The authors [28] of a cross-sectional study investigated the potential exacerbation of the development of disordered eating in bodybuilders (professional and recreational) and strength athletes. The Eating Attitude Test 26 (EAT-26) and the Three-Factor Eating Questionnaire (TFEQ-R21) were used to assess disordered eating and eating behaviors, respectively. The degree of deviation between perceived ideal body weight and actual body weight was associated with an increased risk of eating disorders. Athletes who desired a lower body weight scored higher on the EAT-26 overall (p = 0.001) and on the dieting (p = 0.01) and bulimia (p = 0.001) subscales. The cognitive restraint and emotional eating scales of the TFEQ-R21 were more pronounced in non-professional athletes (p = 0.01). The emotional eating score was higher in women. Appropriate sport- and gender-specific preventive intervention is needed to reduce the risk of eating disorders in both professional and non-professional bodybuilding athletes.
Starting from the premise that female athletes who participate in sports that emphasize aesthetics are potentially more prone to developing Eating Disorders (ED) and eating disorders (ED), the authors [29] of a study initiated in this direction concluded that female bodybuilding athletes have behaviors associated with ED and ED, as well as a preoccupation with nutritional intake, exercise, and appearance modification strategies.
Bodybuilding has become increasingly popular among men as the male body shape has become a topic of interest in recent decades. Bodybuilders wanted to gain more muscle mass and paid attention to their body shape. Based on this goal, they have a series of rules that include a restrictive diet and an excessive exercise program. Recent research has shown that the desire for a more muscular body shape presents eating behavior problems and body dissatisfaction issues in bodybuilders. In this sense some researchers [30] studied the existence of a relationship between the perception of body image, eating disorders, and muscle dysmorphic disorders in male bodybuilders, the results of the study indicating that the psychopathology of eating disorders is related positive for body dissatisfaction and body dysmorphic disorder in male bodybuilders.
The authors’ findings [31] in a longitudinal to assess the severity and temporal stability of the development of pathological eating, social relationships, increased anxiety, and pathological exercise regimes over a competitive cropping season, suggest that the behavioral strategies of Competitive Bodybuilders (CB) are cyclical, after the competition, the intensity of the behaviors reducing the base levels. Consequently, inferences drawn from cross-sectional data that temporally coherent impaired psychosocial functioning and eating disorder symptomatology may be false positives. Therefore, contextual and temporal factors are important research considerations when assessing CB psycho behaviors.
The authors [32] of another study that investigated the presence of pathological forms of eating behavior and disorders in athletes to verify a newly created questionnaire method focused on their screening, in which sense it was carried out a detailed analysis of one of the most commonly used methods, the EAT-26, which was subsequently reworked into a newly created questionnaire that should meet the criteria for application to a group of competitive athletes, being subsequently verified on a group of athletes from risky sports disciplines. It was distributed among athletes in aesthetic sports, especially among aerobics (gymnastics, sports, and fitness), gymnastics (modern and sports), professional dance, figure skating, and bodybuilding/fitness (classic bodybuilding, bikini fitness, and men’s physique).
Five strong factors (eating control, body weight control, training obsession, appetite, and calorie counting) were identified, which can be defined as common and well-known features in the diet and training regime of competitive athletes. At the same time, the factors found can be defined as essential factors that influence the emergence of disturbed eating behavior or the subsequent development of an eating disorder. The results of the paper corresponded to the opinion of many experts that the sports environment is ideal for covering disturbed eating behavior or eating disorders, and diagnosis in this environment is difficult.
The male public is increasingly concerned with body image, which can lead to the development of behaviors and eating disorders that are extremely harmful to health. The quest for an increasingly muscular body indicates a distortion of reality about the self that generates major changes in the habits and routine of these individuals to seek the desired result. Thus, the authors [33] of a study initiated to identify the risk factors for the development of the disorder among groups with different frequencies in the practice of bodybuilding (sedentary (without physical activity), active (frequency of up to 4 times per week) and very active (more than 5 times per week) identified significant differences for individuals classified as very active, with greater symptoms of muscle dysmorphia, desire to increase body size, greater pathological eating attitudes and frequency of body checking behaviors, more negative body beliefs, greater functional impairment, and internalization of a more muscular body relative to the other two participant groups. The frequency with which individuals practiced weight training appeared to be associated with several factors predisposing them to muscle dysmorphia and harmful behaviors.
Orthorexia Nervosa (ON) describes a pathological obsession with healthy eating to avoid ill health, and in the Swedish context, ON is also understood in terms of unhealthy exercise. Personal trainers (PTs) play an important role in detecting unhealthy behaviors, so the authors [34-44] initiated a study by conducting an interpretive qualitative content analysis and Becker’s Kinds of Deviance model on performing healthy and unhealthy exercises and the presence of orthorexia nervosa (OR) eating behaviors during gym workouts. In contrast to the health norms of fitness professionals (PTs), namely practicing balanced behaviors and contributing to well-being, ON was mainly expressed in terms of effortful behavior and as being excessive and in total control. Certain sports contexts (bodybuilding, fitness competitions, and elite sports) and specific groups (fitness professionals) contribute to complicating PT negotiations due to a norm of competition, performance, and/or profession, making it difficult to determine whether to intervene or not.
These results may suggest the presence of severe symptomatology of eating behavior disorders for some athletes, but additional medical investigations by specialized personnel are necessary considering the non-repeatability of this inventory at an interval of at least 6 months or the intervention by training specific to bodybuilding and fitness by means mental and physical to shape the desired, non-pathological body shape.
During the centralization of the results for each athlete for each item and scale separately, erroneous answers to similar questions were noticed, which could have been avoided if the text had been clearer or read more carefully.
The order of the investigated clinical scales, depending on the value of the rated score, resulting from the statistical processing, respectively, NFC, B, and DAS, coincided in ascending order with the number of thresholds exceeded by athletes on the mentioned scale, most athletes falling under of age in the junior category 4 athletes, followed by 3 athletes in the seniors and 2 in the masters.
The averages of the investigated scales for women did not exceed the threshold quotas established for each investigated scale, above which it is considered that the athletes present specific symptoms, however, 3 athletes, of which one junior and two masters exceeded at least one threshold of the DAS and NFC scales. The bulimia scale did not result in values rated above the threshold, so we can conclude that relevant symptoms of eating behavior disorders were not identified in the athletes participating in the study who practice bodybuilding and fitness.
Female athletes (rated score 44.75) have fewer emotional problems than male athletes (rated score 53.89) with approximately 9 points, a result similar to the results of the general psychological maladjustment scale, while on the exaggerated control scale both females (rated score 52, 81) as well as for males (rated score 53.58), the average rated scores exceeded the critical threshold (51.98), the difference between the scores being lower by one point for sportswomen compared to sportswomen for the values obtained regarding behaviors specific to exaggerated control.
The premise of general psychological maladjustment can be further analyzed for a number of 10 athletes who exceeded the critical threshold, of which 4 juniors, 5 seniors, and 1 masters’ category, however, the average result of the rated scores was below the critical threshold value, which means we can add the fact that for women there were no thresholds exceeded on this scale.
Eating disorder risk was identified in 4 athletes, including 3 juniors (two juniors and one junior) and one senior who scored higher than the critical threshold of the scale.
Most of the exceeded thresholds resulted from the centralization of the results on the interpersonal problems scale, where 17 athletes (6 juniors, 8 seniors, 3 masters) obtained scores above the threshold, of which only two athletes (a junior and another masters’ category), and one another athlete, also from the masters’ category, reached the limit. On this scale, the critical threshold was also exceeded for the average value of the rated scores obtained by the 30 athletes.
Among the 2 athletes, of which a junior and a senior exceeded all the validity thresholds of the Eating Disorders Inventory, results call for further investigation and it is necessary to repeat the test and clarify some statements if their meaning was misinterpreted.
The order of approaching the threshold of the investigated scales, in an ascending sense, related to the averages of the rated scores of the psychological scales, following the statistical processing of the respondents’ results:
1. Fear of maturity 48.10, threshold 51.03, difference between values= 2.93;
2. Low self-esteem 48.74, threshold 60.33=11.59
3. Interoceptive deficits 49.6; threshold 52.97=3.37
4. Personal alienation 49.47, threshold 61.65=12.18
5. Perfectionism 50.62, threshold 54.36=3.74
6. Interpersonal alienation 50.75, threshold 53.27=2.52
7. Interpersonal insecurity 51.31, threshold 52.64=1.33
8. Emotional imbalance 53.30, threshold 58.88=5.58
9. Asceticism 55.63, threshold 49.32=+6.31
Depending on the distance from the threshold, the following dynamics result:
1. Personal alienation 49.47, threshold 61.65=12.18
2. Low self-esteem 48.74, threshold 60.33=11.59
3. Emotional imbalance 53.30, threshold 58.88=5.58
4. Interoceptive deficits 49.6; threshold 52.97=3.37
5. Perfectionism 50.62, threshold 54.36=3.74
6. Fear of maturity 48.10, threshold 51.03, difference between values = 2.93
7. Interpersonal alienation 50.75, threshold 53.27 = 2.52
8. Interpersonal insecurity 51.31, threshold 52.64 = 1.33
9. Asceticism 55.63, threshold 49.32 = +6.31
Pros
Used as a screening tool for the presence or predisposition to the development of eating disorders, EDI-III, for knowledge and specialized intervention if necessary, the inventory can be a predictor, a selection factor of future champions, as well as a way to psychological intervention if the symptomatology is specific to competition preparation to optimize sports performance. The complex assessment of personality through the large number of psychological scales investigated by the application of the EDI-III can supplement or confirm the result of the application of other psychological tests.
Cons
The study period coincided with the restriction of freedom of movement and socialization due to the COVID-19 epidemic, an aspect that could have influenced the relatively high scores on interpersonal problems and exaggerated control scales. The relatively small number of participants, different periods of preparation for participating in bodybuilding and fitness competitions, and a large number of items with direct questions that require good self-knowledge, introspection, and desirability in choosing answers.
- Horghidan V. Problematica pshimotricității. București: Globus. 2000.
- Golu M. Bazele psihologiei generale.The basics of general psychology. București: Universitară. 2005.
- Pelin F, Radu P, Mitrache G, Alexandra P. Discobolul - Jurnalul de educație fizică, sport și kinetoterapie. Caracteristici mentale ale atletilor de nivel superior. 2020; 59(1):5-14. doi: https://doi.org/10.35189/dpeskj.2020.59.1.1
- Mihăiță E. Study on aspects of bodybuilding and fitness practitioner's motivation and weight training routine. American Journal of Biomedical Science @ Research. 2023; 19(3):77-97. doi:10.34297/AJBSR.2023.19002553
- Harmanci BS, Okray Z. Body Image, Muscle Dysmorphia and Narcissistic Characteristics of Bodybuilder Males in TRNC. Cyprus Turkish Journal of Psychiatry and Psychology. 2021; 3(2):82-90. doi:10.35365/ctjpp.21.2.09
- Cafri G, Thompson JK, Ricciardelli L, McCabe M, Smolak L, Yesalis C. Pursuit of the muscular ideal: Physical and psychological consequences and putative risk factors. Clin Psychol Rev. 2005 Feb;25(2):215-39. doi: 10.1016/j.cpr.2004.09.003. Epub 2004 Dec 30. PMID: 15642647.
- Parish. Becoming Competitive Amateur Bodybuilders: Identification of Contributors. Psychology of Men & Masculinity. 2010; 11(2):152-159. doi:10.1037/a0018091
- Cook R, Griffiths M, Pontes H. Personality Factors in Exercise Addiction: A Pilot Study Exploring the Role of Narcissism, Extraversion, and Agreeableness. INTERNATIONAL JOURNAL OF MENTAL HEALTH AND ADDICTION. 2020; 18(1):89-102. doi:10.1007/s11469-018-9939-z
- Macho J, Mudrak J, Slepicka P. Enhancing the Self: Amateur Bodybuilders Making Sense of Experiences With Appearance and Performance-Enhancing Drugs. Front Psychol. 2021 Jun 11;12:648467. doi: 10.3389/fpsyg.2021.648467. PMID: 34177704; PMCID: PMC8232052.
- Bridges T. Gender Capital and Male Bodybuilders. BODY & SOCIETY. 2009; 15(1):83-107. doi:10.1177/1357034X08100148
- Marzano-Parisoli M. The contemporary construction of a perfect body image: Bodybuilding, exercise addiction, and eating disorders. QUEST. 2001; 53(2):216-230.
- Clausen L, Rosenvinge JH, Friborg O, Rokkedal K. Validating the Eating Disorder Inventory-3 (EDI-3): A Comparison Between 561 Female Eating Disorders Patients and 878 Females from the General Population. J Psychopathol Behav Assess. 2011 Mar;33(1):101-110. doi: 10.1007/s10862-010-9207-4. Epub 2010 Oct 19. PMID: 21472023; PMCID: PMC3044826.
- Garner DM, Miclea Ș, Joja O-DA. EDI-3, Inventarul tulburărilor de comportament alimentar - 3 Manula de specialitate. Adaptarea și standardizarea EDI-3 pe populația din România. Cluj-Napoca: S.C.Cognitrom S.R.L. 2010.
- Miclea M, Cotârlea P, Nicule C, Sălajan R. CAS++ COGNITROM ASSESSMENT SYSTEM++. Manual de utilizare a aplicației CAS++ 2017. Cluj-Napoca: ASCR 2017. 2017.
- Phoenix C. Auto-photography in aging studies: Exploring issues of identity construction in mature bodybuilders. JOURNAL OF AGING STUDIES. 2010; 24(3):167-180. doi:10.1016/j.jaging.2008.12.007
- Sawicki K. Bodybuilding as a subcultural lifestyle of peripheral youth. HEALTH RISK & SOCIETY. 2016; 18(5-6): 283-300. doi:10.1080/13698575.2016.1211256
- Bjørnestad J, Kandal Ø, Anderssen N. Vulnerable discipline: experiences of male competitive bodybuilders. J Health Psychol. 2014 Sep;19(9):1174-84. doi: 10.1177/1359105313485485. Epub 2013 May 16. PMID: 23682065.
- de Liz CM, Viana Md, Dominski FH, Andrade A. Physical exercise in gyms: perspectives of the self-determination theory. Iberoamerican journal of exercise and sport psychology. 2018; 13(2):235-243. doi:WOS:000436185800008
- Moreno-Murcia JA, Silva BF, Pardo MPJ, Rodriguez SAC, Hernandez HE. Motivation, frequency, and activity type in physical exercise participants. International journal of medicine and science of physical activities and sports. 2012; 12(48):649-662. doi:WOS:00313271700004
- Ibarzabal F, Tubio J. Personality traits in bodybuilders and relationships with anthropometric variables and sport behavior. Journal of Sports Psychology. 2008; 17(1):85-102. doi:WOS:000257792900006
- Lantyer MB, Pietschmann RE, Maynard Dd. Bodybuilding athletes: development of eating disorders after competitions. RBNE-REVISTA BRASILIERA DE NUTRICAO ESPORTIVA. 2023; 17(102):22-31. doi:WOS:000938847800003
- Chappell AJ, Simper T, Barker ME. Nutritional strategies of high level natural bodybuilders during competition preparation. J Int Soc Sports Nutr. 2018 Jan 15;15:4. doi: 10.1186/s12970-018-0209-z. PMID: 29371857; PMCID: PMC5769537.
- Maier MJ, Haeussinger FB, Hautzinger M, Fallgatter AJ, Ehlis AC. Excessive bodybuilding as pathology? A first neurophysiological classification. World J Biol Psychiatry. 2019 Oct;20(8):626-636. doi: 10.1080/15622975.2017.1395070. Epub 2017 Nov 15. PMID: 29057722.
- Abras H, Erdag D, Buran A. Investigation of the Relationship between Muscle Dysmorphia Disorder, Orthorexia Nervosa, and Motivation in Male Individuals Engaged in Bodybuilding Sports. CYPRUS TURKISH JOURNAL OF PSYCHIATRY AND PSYCHOLOGY. 2023; 4(1):13-22. doi:10.35365/ctjpp.22.1.02
- Whitehead J, Slater G, Wright H, Martin L, O'Connor H, Mitchell L. Disordered eating behaviours in female physique athletes. Eur J Sport Sci. 2020 Oct;20(9):1206-1214. doi: 10.1080/17461391.2019.1698659. Epub 2019 Dec 12. PMID: 31771429.
- Steele IH, Pope HG Jr, Kanayama G. Competitive Bodybuilding: Fitness, Pathology, or Both? Harv Rev Psychiatry. 2019 Jul/Aug;27(4):233-240. doi: 10.1097/HRP.0000000000000211. PMID: 31219882.
- Cerea S, Giraldo M, Caudek C, Bottesi G, Paoli A, Ghisi M. Validation of the Muscle Dysmorphic Disorder Inventory (MDDI) among Italian Women Practicing Bodybuilding and Powerlifting and in Women Practicing Physical Exercise. INTERNATIONAL JOURNAL OF ENVIRONMENTAL RESEARCH AND PUBLIC HEALTH. 2022; 19(15). doi:10.3390/ijerph19159487
- Efthymiou D, Kokokiris L, Mesiari C, Vassilopoulou E. Perceived ideal body weight exacerbates bulimia and dieting in Bodybuilding Athletes. Toxicol Rep. 2021 Oct 11;8:1777-1782. doi: 10.1016/j.toxrep.2021.10.007. PMID: 34712596; PMCID: PMC8528646.
- Money-Taylor E, Dobbin N, Gregg R, Matthews J, Esen O. Differences in attitudes, behaviours, and beliefs towards eating between female bodybuilding athletes and non-athletes, and the implications for eating disorders and disordered eating. SPORT SCIENCE FOR HEALTH. 2022; 67-74. doi:10.1007/s11332-021-00775-2
- Devrim A, Bilgic P, Hongu N. Is There Any Relationship Between Body Image Perception, Eating Disorders, and Muscle Dysmorphic Disorders in Male Bodybuilders? Am J Mens Health. 2018 Sep;12(5):1746-1758. doi: 10.1177/1557988318786868. Epub 2018 Jul 13. PMID: 30003837; PMCID: PMC6142149.
- Suffolk MT, Dovey TM, Goodwin H, Meyer C. Psychobehavioral characteristics of competitive bodybuilders: A longitudinal study. INTERNATIONAL JOURNAL OF SPORT PSYCHOLOGY. 2015; 46(2):117-136. doi:10.7352/IJSP2015.46.117
- Stackeová D, Barešová T, Přibylová B. A pilot study of a modification EAT-26 questionnaire for screening pathological eating behavior in competitive athletes. Front Psychol. 2023 Jun 2;14:1166129. doi: 10.3389/fpsyg.2023.1166129. PMID: 37333604; PMCID: PMC10272717.
- Theodoro PB, Manochio-Pina MG, Junqueira AC, Melo Ad. Muscle dysmorphia and risk factors in bodybuilders. RBNE-REVISTA BRASILIERA DE NUTRICAO ESPORTIVA. 2022; 16(100):287-296. doi:WOS:000886221400007
- Haman L, Lindgren E-C, Prell H. "If it's not Iron it's Iron f*cking biggest Ironman": personal trainers' views on health norms, orthorexia and deviant behaviours. INTERNATIONAL JOURNAL OF QUALITATIVE STUDIES ON HEALTH AND WELL-BEING, 12(Supplement 2). 2017. doi:10.1080/17482631.2017.1364602
- Bompa TO, Haff GG. Periodization.Training theory and methodology. Bucharest: Ad Point Promo. 2014.
- De La Poza E, Jodar L, Alkasadi M. Modelling the propagation of adult male muscle dysmorphia in Spain: economic, emotional and social drivers. APPLIED ECONOMICS. 2015; 47(12):1159-1169. doi:10.1080/00036846.2013.870657
- Gargari BP, Khadem-Haghighian M, Taklifi E, Hamed-Behzad M, Shahraki M. Eating attitudes, self-esteem, and social physique anxiety among Iranian females who participate in fitness programs. JOURNAL OF SPORTS MEDICINE AND PHYSICAL FITNESS. 2010; 79-84. doi:WOS:000278330400012
- Levinson CA, Fewell L, Brosof LC. My Fitness Pal calorie tracker usage in the eating disorders. Eat Behav. 2017 Dec;27:14-16. doi: 10.1016/j.eatbeh.2017.08.003. Epub 2017 Aug 18. PMID: 28843591; PMCID: PMC5700836.
- Mangweth-Matzek B, Decker B, Erschbaumer I, Wurnig V, Kemmler G, Bichler CS, Rupp C. Disordered eating symptoms in Austrian men of different ages in the context of fitness centers. EATING AND WEIGHT DISORDERS-STUDIES ON ANOREXIA BULIMIA. 2022; 27(5):1765-1773. doi:10.1007/s40519-021-01317-y
- Parreño-Madrigal IM, Díez-Fernández A, Martínez-Vizcaíno V, Visier-Alfonso ME, Garrido-Miguel M, Sánchez-López M. Prevalence of Risk of Eating Disorders and its Association with Obesity and Fitness. Int J Sports Med. 2020 Sep;41(10):669-676. doi: 10.1055/a-1152-5064. Epub 2020 Jun 2. PMID: 32485780.
- Predoiu R. Sports psychology and performance makers. Caracal: Hoffman. 2021.
- Selenius S, Birgegård A, Forsén Mantilla E. Preliminary evaluation of the online course "I Care" targeting eating disorder knowledge and attitudes among sports coaches and fitness instructors. J Eat Disord. 2022 Sep 29;10(1):142. doi: 10.1186/s40337-022-00663-1. PMID: 36175946; PMCID: PMC9520860.
- Wons O, Lampe E, Patarinski AG, Schaumberg KB, Juarascio A. Perceived influence of wearable fitness trackers on eating disorder symptoms in a clinical transdiagnostic binge eating and restrictive eating sample. EATING AND WEIGHT DISORDERS-STUDIES ON ANOREXIA BULIMIA. 2022; 3367-3377. doi:10.1007/s40519-022-01466-8
- Computerized Psychological Assessment Platform (CAS++). 2023. https://www.cognitrom.ro/produs/evaluare-psihologica/ https://www.cognitrom.ro/download-pdf/3534/